
Abstract
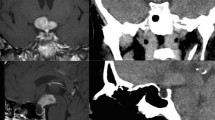
Hypopituitarism can be caused by tumor, inflammation, granuloma and injuries. Once pituitary function is disturbed, hormone replacement therapy is necessary for the remaining life span in most cases. We have experienced a rare case of a unique intrasellar mass associated with pituitary dysfunction in which both spontaneously reversed. A 61-yr-old woman developed hypoadrenalism and central diabetes insipidus (cDI). Magnetic resonance (MR) imaging revealed a lobular, strong hypointense lesion with spotty signal in the middle of the hypophysis. This spotty lesion showed isointensity on T1- and high-intensity on T2-weighted MR images. The spotty signal as well as the normal pituitary lobe were enhanced by the administration of gadolinium. As replacement therapies for hypoadrenalism and cDI, 10 mg of hydrocortisone and 2.5 μg of desmopressin acetate were prescribed. Three months later, slight shrinkage of intrasellar mass and spontaneous improvement of pituitary functions were found. Hydrocortisone was then discontinued. Furthermore, because polyuria and polydipsia were improved nine months later, desmopressin acetate was stopped. Currently, the intrasellar mass continues to shrink, and the patient shows no symptoms without medication. Based upon the unique features of MR images, we suspect that the origin of the mass is an intrasellar hemangioma.
Similar content being viewed by others


References
Dahnert W. Radiology Review Manual. 4th ed. Philadelphia: Lippincott Williams and Wilkins. 2000, 198–99.
Benvenga S, Campenni A, Ruggeri RM, Trimarchi F. Hypopituitarism secondary to head trauma. J Clin Endocrinol Metab 2000, 85: 1353–61.
Benvenga S, Vigo T, Ruggeri RM, et al. Severe head trauma in patients with unexplained central hypothyroidism. Am J Med 2004, 116: 767–71.
Iglesias P, Gomez-Pan A, Diez JJ. Spontaneous recovery from post-traumatic hypopituitarism. J Endocrinol Invest 1996, 19: 320–3.
Barrande G, Kujas M, Gancel A. Granular cell tumors. Rare tumors of the neurohypophysis. Presse Med 1995, 24: 1376–84.
Cone L, Srinivasan M, Romanul FC. Granular cell tumor (Choristoma) of the nerurohypophysis: two cases and a review of the literature. Am J Neuroradiol 1990, 11: 403–6.
Iglesias A, Arias M, Brasa J, Paramo C, Conde C, Fernandez R. MR imaging findings in granular cell tumor of the neurohypophysis: a difficult preoperative diagnosis. Eur Radiol 2000, 10: 1871–3.
Lafitte C, Aesch B, Henry-Lebras F, Fetissof F, Jan M. Granular cell tumor of the pituitary stalk. J Neurosurg 1994, 80: 1103–7.
Buonaguidi R, Canapicci R, Mimassi N, et al. Intrasellar cavernous hemangioma. Neurosurgery 1984, 14: 732–4.
Mitsuhashi T, Hashimoto R, Nagahama S, et al. Intrasellar cavernous angioma in neurofibromatosis. Hum Pathol 1991, 22: 623–4.
Sansone ME, Liwnicz BH, Mandybur TI. Giant pituitary cavernous hemangioma. J Neurosurg 1980, 53: 124–6.
Cobbs CS, Wilson CB. Intrasellar cavernous hemanigoma. J Neurosurg 2001, 94: 520–2.
Shi J, Hang C, Pan Y, et al. Cavernous hemangiomas in the cavernous sinus. Neurosurgery 1999, 45: 1308–14.
Iwai Y, Yamanaka K, Nakajima H, et al. Stereotactic radio-suregeryfor cavernous sinus cavernous hemanigoma. Neurol Med Chir (Tokyo) 1999, 39: 288–90.
Arafah BM, Kailani SH, Nekl KE, Gold RS, Selman WR. Immediate recovery of pituitary function after transsphenoidal resection of pituitary macroadenoma. J Clin Endocrinol Metab 1994, 79: 348–54.
Otsuka F, Ogura T, Hayakawa N, Harada S, Kageyama J, Makino H. reversible hypopituitarism in empty sella syndrome: a case report. Endocr J 1998, 45: 385–91.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Nagai, S., Shimizu, C., Kimura, Y. et al. A case of reversed pituitary dysfunction with intrasellar mass. J Endocrinol Invest 29, 367–372 (2006). https://doi.org/10.1007/BF03344111
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/BF03344111