
Abstract
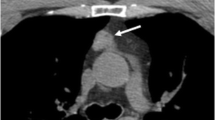
In 1990, a 55-yr-old woman was admitted to the Medical Department of our hospital for severe hypercortisolism complicated by secondary diabetes mellitus and serious hypokalemia. Although inferior petrosal sinus sampling did not show any significant difference between central and peripheral ACTH concentration, suggesting an ectopic source of ACTH secretion, diagnostic imaging was negative and Cushing’s disease due to hyperplasia of the pituitary intermediate lobe was suspected. Medical treatment with bromocriptine and cyproheptadine led to a rapid and stabile normalization of adrenal function, so that after two months cyproheptadine was stopped and bromocriptine was tapered to a smaller dose. An attempt to discontinue medical treatment, carried out 3 yr later, was followed by a quick increase of ACTH and cortisol levels, which were normalized by the resumption of the bromocriptine. Adrenal function remained normal until 1994 when hypercortisolism relapsed despite the treatment. Chest radiography and computed tomography (CT) scan detected a 6 mm nodule in the middle lobe of the lung which proved to be a neuroendocrine tumor, with immunohistochemical positivity for ACTH. Nests of neuroendocrine cells (tumorlets) were also demonstrated in the surrounding lung tissue. After the lobectomy, the patient recovered completely from Cushing’s syndrome and no symptoms and/or signs of recurrence have been observed over the subsequent follow-up period. Although cyclical spontaneous Cushing’s syndrome could not be excluded, there was strong evidence that medical treatment with bromocriptine might have played a key role in long-lasting remission. To our knowledge, this is the second case described in literature of Cushing’s syndrome caused by neuroendocrine lung tumor responsive to bromocriptine.
Similar content being viewed by others

References
Carpenter PC. Diagnostic and evaluation of Cushing’s syndrome. Endocrinol Metab Clin North Am 1988, 17: 445–72.
Thorner MO, Martin WH, Ragan GE, et al. A case of ectopic ACTH syndrome: diagnostic difficulties caused by intermittent hormone secretion. Acta Endocrinol (Copenh) 1982, 99: 364–70.
Findling JW, Tyrrel JB. Occult ectopic secretion of corticotropin. Arch Intern Med 1986, 146: 929–33.
Wajchenberg BL, Mendonca BB, Liberman BM, et al. Ectopic adrenocorticotropic hormone syndrome. Endocr Rev 1994, 15: 752–87.
Lamberts SW, de Lange SA, Stefanko SZ. Adrenocorticotropin-secreting pituitary adenoms originate from the anterior or intermediate lobe in Cuhing’s disease: differences in the regulation of hormone secretion. J Clin Endocrinol Metab 1982, 54: 286–91.
Mc Nicol AM, Teasdale GM, Beastall GH. A study of cor-ticotroph adenomas in Cushing’s disease: no evidence of intermediate lobe origin. Clin Endocrinol (oxf) 1986, 24: 715–22.
Raffel C, Boggan JE, Eng LF, Davis RL, Wilson CB. Pituitary adenomas in Cushing’s disease: do they arise from the intermediate lobe? Surg Neurol 1988, 30: 125–30.
Reith P, Monnot EA, Bathija PJ. Prolonged suppression of a corticotropin-producing bronchial carcinoid by oral bromocriptine. Arch Intern Med 1987, 147: 989–91.
Lemmer K, Ahnert-Hilger G, Hopfner M, et al. Expression of dopamine receptors and transporter in neuroendocrine gastrointestinal tumor cells. Life Sci 2002, 71: 667–78.
Ishibashi M, Fujisawa M, Furue H, Maeda Y, Fukayama M, Yamaji T. Inhibition of growth of human cell lung cancer by bromocriptine. Cancer Res 1994, 4: 3442–6.
Farrel WE, Clark AJ, Stewart MF, Crosby SR, White A. Bromocriptine inhibits pro-opiomelonocortin mRNA and ACTH precursor secretion in small cell lung cancer cell lines. J Clin Invest 1992, 90: 705–10.
Bailey RE. Periodic hormonogenesis. Periodicity of a hormone producing tumor in man. J Clin Endocrinol Metab 1971, 32: 317–27.
Shapiro MS, Gutman A, Bruderman I, Myers B, Griffel WB. Cushing’s syndrome associated with a bronchial adenoma. Possible periodic hormonogenesis. Isr J Med Sci 1975, 11: 919–24.
Chajek T, Romanoff H. Cushing syndrome with cyclical edema and periodic secretion of corticosteroid. Arch Intern Med 1976, 136: 441–3.
Arnaldi G, Mancini T, Kola B, et al. Cyclical Cushing’s syndrome in a patientwith a bronchial neuroendocrinetumor (typical carcinoid) expressing ghrelin and growth hormone secretagogue receptors. J Clin Endocrinol Metab 2003, 88: 5834–40.
Watanobe H, Aoki R, Takebe K, Nakazono M, Kudo M. In vivo and in vitro studies in a patientwith cyclic Cushing’s disease showing some responsiveness to bromocriptine. Horm Res 1991, 36: 227–34.
Rodgers-Sullivan RF, Weiland LH, Palumbo PJ, Hepper MG. Pulmonary tumorlets associated with Cushing’s syndrome. Am Rev Respir Dis 1978, 117: 799–806.
Ranchod M. The histogenesis and development of pulmonary tumorlets Cancer 1977, 39: 1135–45.
Arioglu E, Doppman J, Gomes M, et al. Cushing’s syndrome caused by corticotropin secretion by pulmonary tumorlets. N Eng J Med 1998, 339: 883–6.
Ozbey N, Bozbora A, Kalayci G, et al. Cushing’s syndrome caused by ectopic corticotropin secretion by multiple peripheral pulmonary carcinoids and tumorlets of carcinoid type. J Endocrinol Invest 2000, 23: 536–41.
Povedano ST, Pastor CV, Seoane CP, et al. Ectopic ACTH syndrome caused by pulmonary carcinoid tumourlets. Clin Endocrinol (Oxf) 2001, 54: 839–42.
Liu SM, Wu HH, Wu CJ, Kuo CL, Mo LR. Adrenocorticotropin producing pulmonry tumorlets with lymph node metastasis. PatholInt 2003, 53: 883–6.
Yasuda K, Miura K. Unique type of Cushing’s disease in clinical profile: cyclic Cushing’s syndrome and Cushing’s disease with favorable outcome to high daily dose of bromocriptine. Nippon Naibunpi Gakkai Zasshi 1994, 20: 70.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Francia, G., Davì, M.V., Montresor, E. et al. Long-term quiescence of ectopic Cushing’s syndrome caused by pulmonary neuroendocrine tumor (typical carcinoid) and tumorlets: Spontaneous remission or therapeutic effect of bromocriptine?. J Endocrinol Invest 29, 358–362 (2006). https://doi.org/10.1007/BF03344109
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/BF03344109