
Abstract
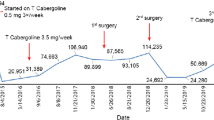
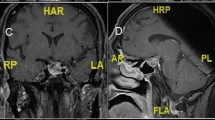
We report the case of a 45-year-old male presenting with unilateral exophthalmos due to a large tumoral mass invading the skull base. Ophthalmologic examination did not show any visual field defects. Imaging techniques demonstrated extension of a huge tumor (approx. 8×8×8 cm) into the right orbit and nasopharynx. Endocrine work-up revealed grossly elevated serum prolactin (PRL) levels (26,466 μg/l, nl. <12), pointing to a large, invasive macroprolactinoma. Stimulation tests indicated associated partial adrenal and growth hormone deficiencies. Planned surgery was abandoned, and the patient was instead treated with the long-acting dopamine agonist, cabergoline. Over a period of one year, serum PRL dropped to 131 μg/l, while the tumor mass shrank to less than 50% of its original volume (with 3.5 mg/ week of cabergoline). The exophthalmos disappeared, and the patient did not develop rhinorrhea or any other side effects from treatment with cabergoline. The efficacy was maintained throughout the second year (ultimate serum PRL 74 μg/l, and final size less than 10% of the original). With reference to this case, we review other macroprolactinomas reported in the recent literature for associated exophthalmos, grossly elevated serum PRL levels (≥15,000 μg/l), and/or “giant” size (≥4 cm in maximum diameter). We highlight the use of dopamine agonists in the treatment of prolactinomas with such unusual characteristics.
Similar content being viewed by others

References
Verhelst J., Abs R., Maiter D., van den Bruel A., Vandeweghe M., Velkeniers B., Mockel J., Lamberigts G., Petrossians P., Coremans P., Mahler C., Stevenaert A., Verlooy J., Raftopoulos C., Beckers A. Cabergoline in the treatment of hyperprolactinemia: a study in 455 patients. J. Clin. Endocrinol. Metab. 1999, 84: 2518–2522.
Murphy F.Y., Vesely D.L., Jordan R.M., Flanigan S., Kohler P.O. Giant invasive prolactinomas. Am. J. Med. 1987, 83: 995–1002.
Davis J.R.E., Sheppard M.C., Heath D.A. Giant invasive prolactinoma: a case report and review of nine further cases. Q. J. Med. 1990, 74: 227–238.
Grebe S.K.G., Delahunt J.W., Feek C.M. Treatment of extensively invasive (giant) prolactinomas with bromocriptine. N. Z. Med. J. 1992, 105: 129–131.
Kolodny J., Dluhy R.G. Recurrent prolactinoma and meningioma following irradiation and bromocriptine treatment. Am. J. Med. 1985, 78: 153–155.
Ross R.J.M., McEniery J.M., Grossman A., Doniach I., Besser G.M., Savage M.O. Massive prolactinoma with galactorrhea in a prepubertal boy. Postgrad. Med. J. 1989, 65: 403–406.
Angyal E.A., Lee H-J., Wolansky L.J., Koenigsberger M.R., Nathanson D., Zimmer A.E. Prolactinoma invasion of superior ophthalmic vein: CT and MR findings. J. Comput. Assist. Tomogr. 1993, 17: 964–966.
Levy R.A., Quint D.J. Giant pituitary adenoma with unusual orbital and skull base extension. Am. J. Rad. 1998, 170: 194–196.
Barkan A.L., Chandler W.F. Giant pituitary prolactinoma with falsely low serum prolactin: the pitfall of the “high-dose hook effect”, case report. Neurosurgery 1998, 42: 913–916.
Daita G., Yonemasu Y., Hashizume A. Unilateral exophthalmos caused by an invasive pituitary adenoma. Neurosurgery 1987, 21: 716–718.
Landolt A.M. Cerebrospinal fluid rhinorrhea: a complication of therapy for invasive prolactinomas. Neurosurgery 1982, 11: 395–401.
Clayton R.N., Webb J., Heath D.A., Dunn P.J., Rolfe E.B., Hockley A.D. Dramatic and rapid shrinkage of a massive invasive prolactinoma with bromocriptine: a case report. Clin. Endocrinol. (Oxf.) 1985, 22: 573–581.
Scherrer H., Turpin G., de Gennes J-L., Schaison-Cusin M., Heshmati H.M., Thibierge M., Metzger J. Résultats du traitement par bromocriptine des adénomes à prolactine géants ou expansifs. Ann. Méd. Interne (Paris) 1985, 136: 459–466.
Barrera C.M., Ruiz A., Banks W.A. A giant prolactinoma and the effect of chronic bromocriptine therapy on basal and TRH-stimulated serum prolactin levels. Horm. Res. 1991, 35: 167–169.
van der Lely A-J., Knegt P.P.M., Stefanko S.Z., Tanghe H.L., Singh R., Lamberts S.W. Nasopharyngeal presentation of pituitary tumors: differential diagnosis and treatment. J. Clin. Endocrinol. Metab. 1992, 74: 811–813.
Reuter U., Mehraein S., Arnold G., Lehmann R.A. A “giant” prolactinoma. J. Neurol. Neurosurg. Psychiatry. 1997, 63: 295.
Saeki N., Nakamura M., Sunami K., Yamaura A. Surgical indication after bromocriptine therapy on giant prolactinomas: effects and limitations of the medical treatment. Endocr. J. 1998, 45: 529–537.
Cannavò S., Bartolone L., Blandino A., Spinella S., Galatioto S., Trimarchi F. Shrinkage of a PRL-secreting pituitary macroadenoma resistant to cabergoline. J. Endocrinol. Invest. 1999, 22: 306–309.
Symon L., Jakubowski J., Kendall B. Surgical treatment of giant pituitary adenomas. J. Neurol. Neurosurg. Psychiatry 1979, 42: 973–982.
Pia H.W., Grote E., Hildebrandt G. Giant pituitary adenomas. Neurosurg. Rev. 1985, 8: 207–220.
Majós C., Coll S., Aguilera C., Acebes J.J., Pons L.C. Imaging of giant pituitary adenomas. Neuroradiology 1998, 40: 651–655.
Perani D., Colombo N., Scotti G., Tonon C. Rapid size reduction of giant prolactinoma following medical treatment. J. Comput. Assist. Tomogr. 1984, 8: 131–133.
Iwai Y., Hakuba A., Khosla V.K., Nishikawa M., Katsuyama J., Inoue Y., Nishimura S. Giant basal prolactinoma extending into the nasal cavity. Surg. Neurol. 1992, 37: 280–283.
Cook R.J., Uttley D., Wilkins P.R., Archer D.J., Bell B.A. Prolactinomas in men masquerading as invasive skull base tumours. Br. J. Neurosurg. 1994, 8: 51–55.
Cole D.R., Lees P.D., Armitage M. A good wife, but never a mother... J.R. Soc. Med. 1995, 88: 176P–178P.
Biller B.M.K., Molitch M.E., Vance M.L., Baker Cannistraro K., Davis K.R., Simons J.A., Schoenfelder J.R., Klibanski A. Treatment of prolactin-secreting macroadenomas with the once-weekly dopamine agonist cabergoline. J. Clin. Endocrinol. Metab. 1996, 81: 2338–2343.
Holness R.O., Schlossberg A.H., Heffernan L.P.M. Cerebrospinal fluid rhinorrhea caused by bromocriptine therapy of prolactinoma. Neurology 1984, 34: 111–113.
Hildebrandt G., Zierski J., Christophis P., Laun A., Schatz H., Lancranjan I., Klug N. Rhinorrhea following dopamine agonist therapy of invasive macroprolactinoma. Acta Neurochir. (Wien) 1989, 96: 107–113.
Bronstein M.D., Musolino N.R., Benabou S., Marino R. Cerebrospinal fluid rhinorrhea occurring in long-term bromocriptine treatment of macro-prolactinomas. Surg. Neurol. 1989, 32: 246–249.
Pascal-Vigneron V., Weryha G., Braun M., Morel-Jean J., Bisset S., Leclère J. La rhinorrhée et l’otorrhée: des complications rares du traitement médical des prolactinomes invasifs. Ann. Endocrinol. (Paris). 1993, 54: 347–351.
Ferrari C.I., Abs R., Bevan J.S., Brabant G., Ciccarelli E., Motta T., Mucci M., Muratori M., Musatti L., Verbessem G., Scanlon M.F. Treatment of macroprolactinoma with cabergoline: a study of 85 patients. Clin. Endocrinol. (Oxf.) 1997, 46: 409–413.
Colao A., Di Sarno A., Landi M.L., Cirillo S., Sarnacchiaro F., Facciolli G., Pivonello R., Cataldi M., Merola B., Annunziato L., Lombardi G. Long-term and low-dose treatment with cabergoline induces macroprolactinoma shrinkage. J. Clin. Endocrinol. Metab. 1997, 82: 3574–3579.
Bevan J.S., Webster J., Burke C.W., Scanlon M.F. Dopamine agonists and pituitary tumor shrinkage. Endocr. Rev. 1992, 13: 220–240.
Cannavò S., Curtò L., Squadrito S., Almoto B., Vieni A., Trimarchi F. Cabergoline: a first-choice treatment in patient with previously untreated prolactin-secreting pituitary adenoma. J. Endocrinol. Invest. 1999, 22: 354–359.
Rains C.P., Bryson H.M., Fitton A. Cabergoline: a review of its pharmacological properties and therapeutic potential in the treatment of hyperprolactinaemia and inhibition of lactation. Drugs 1995, 49: 255–279.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Berwaerts, J., Verhelst, J., Abs, R. et al. A giant prolactinoma presenting with unilateral exophthalmos: Effect of cabergoline and review of the literature. J Endocrinol Invest 23, 393–398 (2000). https://doi.org/10.1007/BF03343743
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/BF03343743