
Abstract
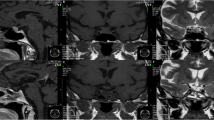
Pituitary apoplexy has been reported as a rare complication of dynamic testing used for the study of pituitary functional reserve. In 1993, a diagnosis of non-secreting macroadenoma with moderate functional hyperprolactinaemia was made in a 43-year-old woman. Soon after the start of therapy with bromocriptine up to 5 mg/die, the patient complained of nausea and postural hypotension. As the symptoms persisted even when the dose was reduced to 2.5 mg/die, the patient was transferred to therapy with quinagolide at the dosage of 37.5 μg/die. PRL levels quickly normalized (range 1.4–5.7 ng/ml) as well as menstrual cycles, and no side-effect was reported. In 1995 a sellar magnetic resonance imaging (MRI) showed no shrinkage of the known macroadenoma. In 1996, few hours after a gonadotropin-releasing-hormone (GnRH) test, which showed normal LH and FSH response and with baseline PRL levels in the normal range, the patient started complaining of severe frontal headache, nausea and vomiting. No gross visual defects were present. An emergency computed tomography (CT) showed no evident hemorrhagic infarction in the macroadenoma. The symptoms completely resolved in few days with steroidal and antiemetic therapy. A new MRI performed in 1998 showed a partial empty sella and PRL levels were in the normal range under do-paminergic treatment. The pituitary functional reserve proved normal on dynamic testing. The temporal association between the onset of symptoms and the GnRH test strongly suggests an association between the two events. No evident signs of pituitary apoplexy (either on emergency CT or hormonal evaluation) were detected. The authors suggest that GnRH can cause severe side-effects that mimic pituitary apoplexy without related morphological evidence and that, in our particular case, it can have caused the gradual disappearance of the non-secreting macroadenoma. Moreover, a causal role of the chronic dopaminergic treatment cannot be completely ruled out.
Similar content being viewed by others


References
Morsi A., Jamal S., Silverberg J.D.H. Pituitary apoplexy after leuprolide administration for carcinoma of the prostate. Clin. Endocrinol. (Oxf.) 1996, 44: 121–124.
Bernstein M., Hegele R.A., Gentili F., Brothers M., Holgate R., Sturtridge W.C., Deck J. Pituitary apoplexy associated with a triple bolus test. J. Neurosurg. 1984, 61: 586–590.
Masson E.A., Atkin S.L., Diver M., White M. Pituitary apoplexy and sudden blindness following the administration of gonadotrophin releasing hormone. Clin. Endocrinol. (Oxf.) 1993, 38: 109–110.
Korsic M., Lelas-Bahun N., Surdonja P., Besenski N., Horvat S., Plavsic V. Infarction of FSH-secreting pituitary adenoma. Acta Endocrinol. (Copenh.) 1984, 107: 149–154.
Drury P.L., Belchetz P.E., McDonald W.I., Thomas D.G.T., Besser G.M. Transient amaurosis and headache after thyrotrophin releasing hormone. Lancet 1982, 1: 218–219.
Rolih C.A., Ober K.P. Pituitary apoplexy. Endocrinol. Metab. Clin. North Am. 1993, 22: 291–302.
Reznik Y., Chapon F., Lahlou N., Deboucher N., Mahoudeau J. Pituitary apoplexy of a gonadotrophin adenoma following gonadotrophin-releasing hormone agonist therapy for prostatic cancer. J. Endocrinol. Invest. 1997, 20: 566–568.
Liuzzi A., Dallabonanza D., Opizzi G., Verde G.G., Cozzi R., Chiodini P., Luccarelli G. Low dose of dopamine agonists in the long-term treatment of macroprolactinomas. N. Engl. J. Med. 1985, 313: 656–659.
Ferone D., Lastoria S., Colao A., Varrella P., Cerbone G., Acampa W., Merola B., Salvatore M., Lombardo G. Correlation of scintigraphic results using 123I-metho-xybenzamide with hormone levels and tumor size response to quinagolide in patients with pituitary adenomas. J. Clin. Endocrinol. Metab. 1998, 83: 248–252.
Shimon I., Melmed S. Management of pituitary tumors. Ann. Intern. Med. 1998, 129: 472–483.
Author information
Authors and Affiliations
Corresponding author
Additional information
This work was presented in part at 3° Simposio Livornese sugli Adenomi Ipofisari, Livorno, Italy, January 29–30, 1999.
Rights and permissions
About this article
Cite this article
Foppiani, L., Piredda, S., Guido, R. et al. Gonadotropin-releasing hormone-induced partial empty sella clinically mimicking pituitary apoplexy in a woman with a suspected non-secreting macroadenoma. J Endocrinol Invest 23, 118–121 (2000). https://doi.org/10.1007/BF03343690
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/BF03343690