
Abstract
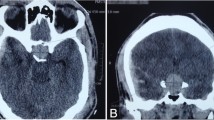
Hypopituitarism (HYPO) is an under-investigated disease in older patients. Symptoms, which may be life-threatening, are aspecific and often attributed to aging and/or related morbidities. We describe here the cases of two elderly patients who were ultimately diagnosed as having HYPO, the clinical presentations and etiologies of which were different. In the first patient, an invasive non-secreting pituitary macroadenoma causing HYPO was detected on brain morphological evaluation for head trauma secondary to falling. Glucocorticoid replacement therapy was started. Thyroid function evaluation showed hyperthyroidism (due to a known toxic multinodular goiter), which was already on treatment with methimazole; ultimately, after withdrawal of the antithyroid drug, secondary hypothyroidism occurred. The patient underwent non-radical pituitary surgery. Cognitive function, gait impairment and falling, which had previously been attributed only to aging, improved markedly after cortisone acetate and L-thyroxine replacement therapy. The second patient was hospitalized one month after the onset of hypotension, edema and pain in the legs, and progressive psychomotor impairment, which ultimately resulted in an intermittent soporous state. She was diagnosed as having global anterior HYPO secondary to empty sella, which caused severe multifaceted clinical and biochemical abnormalities (hyponatremia, pancytopenia, rhabdomyolysis). After treatment with i.v. fluids and hydrocortisone, the patient’s clinical condition and biochemical alterations improved, and normalized over time with oral cortisone acetate and L-thyroxine combination therapy. Several protean symptoms that impair the quality of life of elderly patients are usually ascribed to aging. Such symptoms should be investigated with regard to possible HYPO, treatment of which can result in significant clinical benefit.
Similar content being viewed by others

References
Toogood AA, Stewart PM. Hypopituitarism: clinical features, diagnosis and management. Endocrinol Metab Clin North Am 2008; 37: 235–61.
Schneider HJ, Aimaretti G, Kreitschmann-Andermahr I, Stalla GK, Ghigo E. Hypopituitarism. Lancet 2007; 369: 1461–70.
Vance ML. Hypopituitarism. N Engl J Med 1994; 330: 1651–62.
Prabhakar VKB, Shalet SM. Aetiology, diagnosis, and management of hypopituitarism in adult life. Postgrad Med J 2006; 82: 259–66.
Minniti G, Esposito V, Piccirilli M, Fratticci A, Santoro A, Jaffrain-Rea ML. Diagnosis and management of pituitary tumours in the elderly: a review based on personal experience and evidence of literature. Eur J Endocrinol 2005; 153: 723–35.
Diderich S, Franzen NF, Bähr V, Oelkers W. Severe hyponatremia due to hypopituitarism with adrenal insufficiency: report on 28 cases. Eur J Endocrinol 2003; 148: 609–17.
Chanson P. Severe hyponatremia as a frequent revealing sign of hypopituitarism after 60 years of age. Eur J Endocrinol 2003; 149: 177–8.
Beshyah SA, Johnston DG. Cardiovascular disease and risk factors in adults with hypopituitarism. Clin Endocrinol 1999; 50: 1–15.
Nilsson B, Gustavasson-Kadaka E, Bengtsson BA et al. Pituitary adenomas in Sweden between 1958 and 1991: incidence, survival, and mortality. J Clin Endocrinol Metab 2000; 85: 1420–5.
Tomlinson JW, Holden N, Hills RK et al. Association between premature mortality and hypopituitarism. Lancet 2001; 357: 425–31.
Benvenga S, Campenni A, Ruggeri RM, Trimarchi F. Hypopituitarism secondary to head trauma. J Clin Endocrinol Metab 2000; 85: 1353–61.
Bondanelli M, Ambrosio MR, Zatelli MC, De Marinis L, degli Uberti EC. Hypopituitarism after traumatic brain injury. Eur J Endocrinol 2005; 152: 679–91.
Schneider HJ, Kreitschmann-Andermahr I, Ghigo E, Stalla GK, Agha A. Hypothalamopituitary dysfunction following traumatic brain injury and aneurysmal subarachnoid hemorrhage. JAMA 2007; 298: 1429–38.
Regal M, Páramo C, Sierra JM, García-Mayor RV. Prevalence and incidence of hypopituitarism in an adult Caucasian population in northwestern Spain. Clin Endocrinol 2001; 55: 735–40.
Turner HE, Wass JA. Pituitary tumours in the elderly. Bailliere’s Clin Endocrinol Metab 1999; 11: 407–422.
Johnston S, Hoult S, Chan CA. Falling again. The Lancet 1996; 348: 26.
Cikim A, Dikilitas M, Cikim K. Hypopituitarism in older adults. The report of five cases with different presentations. Geriatrics 2006; 61: 32–5.
Chandler WF, Barkan AL. Treatment of pituitary tumors: a surgical perspective. Endocrinol Metab Clin North Am 2008; 37: 51–66.
Faustini-Fustini M, Anagni M. Beyond semantics: defining hyponatremia in secondary adrenal insufficiency. J Endocrinol Invest 2006; 29: 267–9.
Sasaki M, Yuzawa M, Saito T et al. Clinical and laboratory features of hyponatremia-induced myopathy. Clin Exp Nephrol 2007; 11: 283–6.
Nguyen-Michel VH, Schwald N, Hunert S, Chahwakilian A, Debray-Meignan S. Central hypothyroidism allows discovery of a pituitary disease in older people. J Am Geriatr Soc 2007; 55: 630–1.
Waise A, Belchetz PE. Unsuspected central hypothyroidism. BMJ 2000; 321: 1275–7.
Nishioka H, Haraoka J. Hypopituitarism and anemia: effect of replacement therapy with hydrocortisone and/or levothyroxine. J Endocrinol Invest 2005; 28: 528–33.
Rudzki Z, Matynia A, Przybylik-Mazurek E et al. Hypopituitarism and hematological abnormalities mimicking myelodysplastic syndrome. Report of four cases. Pol Arch Med Wewn 2003; 110: 1003–11.
Nomiyama J, Shinohara K, Inoue H. Improvement of anemia by recombinant erythropoietin in a patient with postoperative hypopituitarism. Am J Hematol 1994; 47: 249–50.
De Marinis L, Bonadonna S, Bianchi A, Maira G, Giustina A. Extensive clinical experience: primary empty sella. J Clin Endocrinol Metab 2005; 90: 5471–7.
Del Monte P, Foppiani L, Cafferata C, Marugo A, Bernasconi D. Primary empty sella: endocrine findings. Endocr J 2006; 53: 803–9.
Jeffcoate W. Assessment of corticosteroid replacement therapy in adults with adrenal insufficiency. Ann Clin Biochem 1999; 36: 151–7.
Ten S, New M, MacLaren N. Addison’s disease 2001. J Clin Endocrinol Metab 2001; 86: 2909–22.
Peacey S, Guo C-Y, Robinson SM et al. Glucocorticoid replacement therapy: are patients over treated and does it matter? Clin Endocrinol 1997; 46: 255–61.
Molitch ME, Clemmons DR, Malozowski S et al. Evaluation and treatment of adult growth hormone deficiency: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab 2006; 91: 1621–34.
Franco C, Johannsson G, Bengtsson BA, Svensson J. Baseline characteristics and effects of growth hormone therapy over two years in younger and elderly adults with adult onset GH deficiency. J Clin Endocrinol Metab 2006; 91: 4408–14.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Foppiani, L., Ruelle, A., Quilici, P. et al. Hypopituitarism in the elderly: two case-reports with heterogeneous presentation. Aging Clin Exp Res 21, 76–81 (2009). https://doi.org/10.1007/BF03324902
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/BF03324902