
Summary
Introduction
Pulmonary embolism, recurrent venous thromboembolism and post-thrombotic syndrome are major effects of deep vein thrombosis. As major orthopedic surgery for hip and knee is an important risk factor for these events, pharmacologic and/or physical prophylaxis is recommended. The study was designed to a) document methods of prophylaxis and estimate associated health care costs borne by the Italian National Health Service (NHS) and by patients who are administered the prophylaxis for hip/knee surgery; b) to detect possible determinants of interruption and/or switch of the therapy commenced during the hospital stay.
Study design
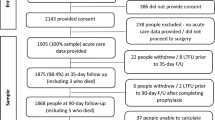
The study is observational and multi-centric. Patients were followed up for two months after discharge or until interruption of the prophylaxis. Data were purposely collected through specific questionnaires administered during patients’ hospitalisation, at each follow-up visit and at completion/interruption of the prophylaxis.
Results
125 patients were enrolled. About 2/3 of the sample were female while 60% were at least 70 years old; average age was 69. Most of the patients underwent hip surgery. Hospital prophylaxis averaged 11.9 days. Forty-one per cent of patients were administered nadroparin, while 40% were administered enoxaparin sodium. The remaining patients (19%) were administered dalteparin. For all treatments daily dosage was 0.4 ml. For most of patients specific training was provided on how to administrate and monitor the prophylaxis. After hospital discharge patients were either sent home (57.6%) or sent to a rehabilitation centre (42.4%). All patients remained on therapy; however, 10% changed therapy and another 3% prematurely ceased treatment. Mean stay on therapy after hospital discharge was 33 days. Total prophylaxis costs averaged 355 Euro. Fifty-six per cent of costs was for the drug, while 41% is attributable to the value of the time spent by professionals and caregivers to administer the treatment. Average daily cost per patient was 8 Euro (range: 2.7–14.3 Euro). Total cost high variability is mainly attributable to the duration of the prophylaxis which, in turn, is dependent on the setting of administration. In these patients, anti-thrombotic prophylaxis poses a relevant economic burden both to the NHS and to patients and their caregivers.
Similar content being viewed by others


Bibliografia
Nicolaides AN. Consensus Statement. Prevention of venus thromboembolism. Int Angiol 1997; 16: 3–38
Second Thromboembolic Risk Factors (THRiFT II) Consensus Group. Risk and prophylaxis for venous thromboembolism in hospital patients. Phlebologie 1998; 13: 87–97
Geerts WH, Heit JA, Clagett GP, et al. Sixth ACCP Consensus Conference on antithrombotic therapy. Prevention of venous thromboembolism. Chest 2001; 119 (Suppl.): 132S–75S
Prevention of venous thromboembolism: European consensus statement. Developed under the auspices of the Cardiovascular Disease Education and Research Trust; 1991 Nov 1–5; Windsor. Cyprus: Med-Orion Publishing Company, 1992
Oster G, Tuden R, Colditz A. A cost-effectiveness analysis of prophylaxis against deep vein thrombosis in major orthopedic surgery. JAMA 1987; 157(2): 203–8
Hyers TM, Management of venous thromboembolism. Past, present and future. Arch Intern Med 2003; 163: 759–68
Botterman MF, Caprini J, Stephens, et al. Results of an economic model to assess the cost-effectiveness of enoxaparin, a low molecular weight heparin, versus warfarin for the prophylaxis of deep vein thrombosis and associated long-term complications in total hip replacement surgery in the United States. Clin Ther 2002; 24(11): 1960–86
Wade WE, Hawkins DW. Cost Effectiveness of outpatient anticoagulant prophylaxis after total hip arthroplasty. Orthopedics 2000; 23(4): 335–9
Sullivan SD, Kahn SR, Davidson BL, et al. Measuring the outcome and pharmacoeconomic consequences of venous thromboembolism prophylaxis in major orthopedic surgery. Pharmacoeconomics 2003; 21(7): 477–96
Marchetti M, Liberato NL, Ruperto N, et al. Long-term cost-effectiveness of low molecular weight heparin versus unfractionated heparin for the prophylaxis of venous thromboembolism in elective hip replacement. Haematologica 1999; 84: 730–37
Anderson Jr FA, Wheeler HB, Goldberg RJ, et al. A population-based perspective of the hospital incidence and case-fatality rates of deep vein thrombosis and pulmonary embolism. The Worcester DVT study. Arch Intern Med 1991; 151: 933–8
Rosendal FR. Thrombosis in the young: epidemiology and risk factors. A focus on venous thrombosis. Thromb Haemost 1997; 78: 1–6
Nordström M, Lidblad B, Bergqvist D, et al. A prospective study of the incidence of deep-vein thrombosis within a defined urban population. J Intern Med 1992; 232: 155–60
Attanasio E, Russo P, Carunchio G, et al. Dermatan sulfate versus unfractionated heparin for the prevention of venous thromboembolism in patients undergoing surgery for cancer: A cost effectiveness analysis. Pharmacoeconomics 2001: 19(1): 57–68
Menzin J, Colditz GA, Regan MM, et al. Cost-effectiveness of enoxaparin versus low-dose warfarin in the prevention of deep-vein thrombosis after total hip replacement surgery. Arch Intern Med 1995; 155: 757–63
Lloyd A, Aitken JA, Hoffmeyer UKO, et al. Economic evaluation of the use of nadroparin calcium in the prophylaxis of deep vein thrombosis and pulmonary embolism in surgical patients in Italy. Pharmacoeconomics 1997; 12(4): 475–85
Drummond M, Aristides M, Davies L, et al. Economic evaluation of standard heparin and enoxaparin for prophylaxis against deep vein thrombosis in elective hip surgery. Br J Surg 1994; 81: 1742–6
Borris LC, Lassen MR. Thromboprophylaxis with low molecular weight heparin after major orthopaedic surgery is cost effective. Drugs 1996; 52 (Suppl. 7): 42–6
Hawkins DW, Langley PC, Krueger KP. Pharmacoeconomic model of enoxaparin versus heparin for prevention of deep vein thrombosis after total hip replacement. Am J Health Syst Pharm 1997; 54(10): 1185–90
O’Brien BJ, Anderson DR, Goeree R. Cost-effectiveness of enoxaparin versus warfarin prophylaxis against deep-vein thrombosis after total hip replacement. CMAJ 1994; 150: 1083–90
Hull RD, Raskob GE, Pineo GF, et al. Subcutaneous low-molecular-weight heparin vs warfarin for prophylaxis of deep vein thrombosis after hip or knee implantation: an economic perspective. Arch Intern Med 1997; 157: 298–303
Saunders M, Grant R. Cost-effectiveness of low-molecular weight heparin versus warfarin following hip replacement surgery. J Natl Med Assoc 1998; 90: 677–80
Drummond MF, Stoddart GL, Torrance GW. Methods for the economic evaluation of health care programmes. New York: Oxford University Press, 1997
Gold MR, Siegel JE, Russel LB, et al. Cost-effectiveness in health and medicine. New York: Oxford University Press, 1996
L’Informatore Farmaceutico. Milano: OEMF, 2002
Legge 112/02 “Conversione in legge, con modificazioni, del decreto-legge 15 aprile 2002, n. 63, recante disposizioni finanziarie e fiscali urgenti in materia di riscossione, razionalizzazione del sistema di formazione del costo dei prodotti farmaceutici, adempimenti ed adeguamenti comunitari, cartolarizzazioni, valorizzazione del patrimonio e finanziamento delle infrastrutture”
ARAN, Contratto Collettivo Nazionale del lavoro comparto sanità. II biennio economico 2000–2001
IPASVI, Nomenclatore Tariffario 2002 Prestazioni di assistenza infermieristica approvato dal Consiglio Nazionale della Federazione dei Collegi IPASVI il 3 marzo 2002
Ministero della Sanità. Prestazioni di assistenza specialistica ambulatoriale erogabili nell’ambito del SSN e relative tariffe. Decreto Ministeriale del 22 luglio 1996
Lucioni C. Il costo sociale del diabete di tipo 2 in Italia: lo studio CODE-2. Pharmacoeconomics-Italian Research Articles 2000; 2(1): 1–21
Comp PC, Spiro TE, Friedman RJ, et al. Prolonged enoxaparin therapy to prevent venous thromboembolism after primary hip or knee replacement. J Bone Joint Surg 2001; 83A(3): 337–45
Hull RD, Pineo GF Stein PD, et al. Extended out of hospital low-molecular-weight heparin prophylaxis against deep venous thrombosis in patient after elective hip arthroplasty: a systematic review. Ann Intern Med 2001; 135: 858–69
Leclerc JR, Gent M, Hirsh J, et al. The incidence of symptomatic venous thromboembolism during and after prophylaxis with enoxaparin: a multi-institutional cohort study of patients who underwent hip or knee arthroplasty. Canadian Collaborative Group. Arch Intern Med 1998; 158: 873–8
Colwell Jr CW, Collis DK, Paulson R, et al. Comparison of enoxaparin and warfarin for the prevention of venous thromboembolic disease after total hip arthroplasty: evaluation during hospitalization and three months after discharge. J Bone Joint Surg Am 1999; 81: 932–40
Author information
Authors and Affiliations
Corresponding author
Additional information
La dott.ssa Elisa Martelli ha contribuito alla progettazione e conduzione dello studio quando era ricercatrice del CeRGAS.
Rights and permissions
About this article
Cite this article
Fattore, G., Colangelo, I., Martelli, E. et al. Metodi e costi della profilassi della trombosi venosa profonda in chirurgia ortopedica in Italia. Pharmacoeconomics-Ital-Res-Articles 6, 69–80 (2004). https://doi.org/10.1007/BF03320625
Published:
Issue Date:
DOI: https://doi.org/10.1007/BF03320625