
Summary
Objective
Patients with severe heart failure, refractory to drug treatment, can be indicated for biventricular pacing, shown to be useful in overcoming the desynchronization of the ventricular contraction pattern, which generally worsens the hemodynamic conditions of such patients.
This study was aimed at assessing 1) clinical effectiveness of conventional therapy compared with biventricular pacemaker; 2) hospital ward’s budget before and after device implantation.
Methods
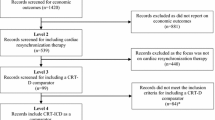
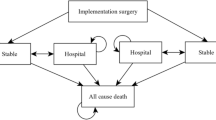
The study was carried out according to an observational method, on 30 patients, retrospectively 1-year before implantation and prospectively 1-year afterwards. The economic analysis was designed and carried out in the hospital perspective. End-points were: Ejection fraction, New York Heart Association (NYHA) class, no. of hospitalizations in Cardiology Ward and ICU (Intensive Care Unit), Days of hospitalization in Cardiology Ward and ICU, no. of clinic visits (outpatients), no. of day-hospital visits, no. of days free from acute events requiring hospitalization or clinic visits, health care costs.
Results
In the 12 months following biventricular pacing, patients showed: a reduction in functional NYHA class (3.0 ± 0.3 vs 2.1 ± 0.3); a reduction in cardiovascular related hospital stays (from 42.0 ± 37.5 days to 2.8 ± 6.4); an increase in number of days free from acute events (from 104 ± 123 to 266 ± 137). Overall costs decreased from € 383,518 to € 289,890 (with implant costs) and to € 58,549 (without implant costs). In-hospital stays in Cardiology and Coronary Unit decreased by 93% and 95%, respectively.
Conclusions
Biventricular pacing in heart failure patients represents an efficient approach in the hospital perspective and allows a less intensive use of clinical resources. Even if other non-hospital-sustained costs are not taken into consideration, it seems reasonable to deduce that the significant improvement in patient’s clinical condition after implantation will provide a considerable reduction of total costs also in a broader perspective.
Similar content being viewed by others

Bibliografia
Schweiger C, Maggioni AP. Scompenso cardiaco ancora in attesa di strategie. Sole 24ore Sanità. 20–26 novembre 2001
Ministero della Salute. Clinical Evidence: una sintesi delle migliori prove di efficacia. Ed. it. Milano; Zadig, 2001
Ministero della Salute. Rapporto sulle schede di dimissione ospedaliera (SDO) 2000. www.ministerodellasalute.it
Gavazzi A. La terapia elettrica nello scompenso cardiaco. Ital Heart J 2002; 3 (suppl. 3): 70S–4S
Ricci R, Ansalone G, Toscano S, et al. Cardiac resynchronization: materials, technique and results. The InSync Italian Registry. Eur Heart J 2000; 2 (suppl J): J6–15
Abraham WT, Fisher WG, Smith AL, et al. Cardiac resynchronization in chronic heart failure. N Engl J Med 2002; 346(24): 1845–53
Alonso C, Leclercq C, Revault D’allonnes F, et al. Six year experience of transvenous left ventricular lead implantation for permanent biventricular pacing in patients with advanced heart failure: technical aspects. Heart 2001; 86: 405–10
Gras D, Leclercq C, Tang ASL, et al. Cardiac resynchronization therapy in advanced heart failure: the multicenter InSync clinical study. Eur J Heart Fail 2002; 4: 311–20
Gasparini M, Curnis A, Daubert JC, et al. Implant feasibility and electrical performance over time of a new left heart side wire lead. Results of a multicenter experience. North American Society of Pacing and Electrophysiology (NASPE), 22nd Annual Scientific Sessions, Boston, May 2–5, 2001. (abstr.)
Cazeau S, Leclercq C, Lavergne T, et al. Effects of multisite biventricular pacing in patients with heart failure and intraventricular conduction delay. N Engl J Med 2001; 344: 873–80
Purerfellner H, Nesser HJ, Winter S, et al. Transvenous left ventricular lead implantation with the EASYTRAK lead system: the European experience. Am J Cardiol 2000; 86 (suppl 1): K157–64
Kervin WF, Botvinick EH, O’Connel JW, et al. Ventricular contraction abnormalities in dilated cardiomiopathy: effect of biventricular pacing to correct interventricular dyssyncrony. J Am Coll Cardiol 2000; 35: 121–7
Auricchio A, Stellbrink C, Sack S, et al. Chronic benefits as a result of pacing in congestive heart failure: results of the PATHCHF trials. Circulation 2000; 102 (18 suppl. II): abstr. 3352A
Abraham WT. Rationale and design of a randomized clinical trial to assess the safety and efficacy of cardiac resynchronization therapy in patients with advanced heart failure: the Multicenter InSync Randomized Clinical Evaluation (MIRACLE). J Card Fail 2000; 6: 369–80
Hare JM. Cardiac-resynchronization therapy for heart failure. N Engl J Med 2002, Editorial; 346(24): 1902–04
Braunschweig F, Linde C, Gadler F, Rydén L. Reduction of hospital days by biventricular pacing. Eur J Heart Fail 2000; 2: 399–406
D.G.R.Lombardia n. VI/38133 del 6 agosto 1998. “Attuazione dell’articolo 12, comma 3 e 4, della L.R. 11.7.1997 n.31. Definizione di requisiti e indicatori per l’accreditamento delle strutture sanitarie”
Apolone G, Brazzi L, Ravizza A, et al. GiViTi — Un gruppo per la terapia intensiva. Torino: Edizioni Minerva Medica, 1996
Chinaglia A, Giaschino G, Asteggiano R, et al. Fattibilità ed efficacia di un programma di assistenza integrata tra ospedale e territorio basata su un ambulatorio infermieristico nella gestione dei pazienti con scompenso cardiaco. Risultati clinici a 6 mesi e costi relativi. Ital Heart J 2002; 3 (suppl. 5): 532–8.
Dixon LJ, Thompson G, Harbinson M, et al. Cardiac resynchronisation therapy — a cost effective treatment for cardiac failure. Eur Heart J 2002; 23 (suppl. August): 3 (abstr.)
Ryden-Bergsten T, Andersson F. The health care costs of heart failure in Sweden. J Int Med 1999; 246: 275–84
DRG Guidebook. A comprehensive reference to the DRG classification system. 16th ed. Ingenix Publishing, USA
Leclerq C, Kass DA. Retiming the failing heart: principles and current clinical status of cardiac resynchronization. J Am Coll Cardiol 2002; 39: 194–201
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Curnis, A., Caprari, F., Mascioli, G. et al. Valutazione economica della resincronizzazione cardiaca nei pazienti affetti da scompenso cardiaco moderato-avanzato. Pharmacoeconomics-Ital-Res-Articles 5, 11–22 (2003). https://doi.org/10.1007/BF03320600
Published:
Issue Date:
DOI: https://doi.org/10.1007/BF03320600