
Summary
Synopsis
Patients with haematological disease, such as leukaemia or aplastic anaemia, may receive bone marrow transplantation (BMT) to improve long term survival. In patients receiving allogeneic BMT, T cells from donor marrow may mount an immunological attack on host tissues (e.g. skin, liver, gastrointestinal tract) and this is manifested as graft versus host disease (GVHD). Indeed, GVHD is associated with significant morbidity and mortality and is the most important complication following allogeneic BMT.
Cyclosporin, an immunosuppressive agent with relatively selective and reversible effects on T helper cells, has been evaluated alone and in combination with methotrexate in a number of clinical trials for the prevention of GVHD in patients receiving allogeneic BMT matched at the major histocompatibility complex from sibling donors. In general, cyclosporin monotherapy achieved similar clinical outcomes to those seen with methotrexate monotherapy in comparative studies; however, cyclosporin has become a cornerstone of GVHD prophylaxis and these drugs are usually administered concomitantly for prevention of GVHD in contemporary clinical practice.
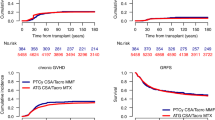
Comparative studies demonstrated a significantly lower incidence of grade II to IV acute GVHD with a combined prophylactic regimen of cyclosporin plus methotrexate than with either drug used alone. The probability of long term survival tended to be or was significantly higher with the combined regimen than with monotherapy.
Patients with established grade II to IV acute GVHD generally do not respond well to therapy. Cyclosporin has not been extensively evaluated informal trials in this clinical setting; however, available data suggest that it is as effective as corticosteroids, which are generally considered to be first- line therapy. Some patients may require combined treatment such as a corticosteroid plus cyclosporin and/or antithymocyte globulin.
In conclusion, cyclosporin appears to be as effective as corticosteroids in treating established GVHD. For prophylaxis of GVHD in patients receiving BMT for haematological disease, cyclosporin is a cornerstone of therapy and is usually used in combination with methotrexate, since their combined use is more effective than either drug used alone. While other strategies for prevention of GVHD have also shown promise, including in vitro T cell depletion of donor marrow, no agent or regimen is ideal, since adverse events, increased leukaemic relapse rates, graft rejection and infection remain important concerns. However, of currently available therapeutic options for prevention of GVHD, the optimal immunosuppressive regimen appears to be a combination of cyclosporin plus methotrexate.
Pharmacodynamic Properties
Cyclosporin is an immunosuppressant that acts primarily through relatively specific and reversible effects on T helper cells, inhibiting production of interleukin-2 which is an integral component of the cellular immune response. Clinical and histological evaluations in animal models of graft versus host disease (GVHD) showed that cyclosporin prevented or reduced the risk of acute GVHD when initiated early [e.g. from the day before bone marrow transplantation (BMT); day —1] but not when therapy was delayed until day 7. A combined prophylactic regimen of cyclosporin from days 0 to 100 plus methotrexate on days 1,3,6 and 11 was associated with long term survival in 4 of 10 animals, compared with no long term survivors when either drug was used alone, in a dog model of GVHD in which bone marrow was mismatched at the major histocompatibility complex. Cyclosporin has had only limited success in treating established experimental GVHD.
Renal dysfunction associated with cyclosporin is generally dose-related and reversible, resulting primarily from functional and structural changes in the proximal tubule and afferent arteriole. The mechanism of these effects appears to be related to a reduction in glomerular filtration rate and a complex multifactorial process involving physiological and intracellular signalling processes.
Pharmacokinetic Properties
Following oral administration of cyclosporin, absorption from the gastrointestinal tract is slow and erratic. Bioavailability ranges widely from 10 to 60%, but is usually about 30%. Peak blood cyclosporin concentrations are achieved 1 to 8 hours after administration and in some patients a second peak may occur 5 to 6 hours later. Recently, a microemulsion-based formulation of cyclosporin (Neoral®) has been developed to overcome problems associated with the poor and variable bioavailability of the standard oral formulations. The microemulsion-based formulation provides more predictable and more extensive cyclosporin absorption than the standard oral formulations. Furthermore, absorption and bioavailability of the microemulsion-based formulation are relatively unaffected by food intake and appear to be almost independent of biliary flow.
Cyclosporin is extensively distributed to tissue sites but does not significantly penetrate the blood-brain barrier. Cyclosporin in whole blood is taken up by erythrocytes and other blood cells, but also distributes into plasma where it is primarily bound to lipoproteins. The drug undergoes extensive metabolism, primarily by the cytochrome P450 3A enzyme system in the liver, and more than 30 metabolites have been identified (some with modest immunosuppressive activity). Elimination half-life in blood ranges from 2.9 to 19 hours. More than 90% of an administered dose is excreted in the bile (<1% as unchanged cyclosporin).
Therapeutic Efficacy
In general, randomised prospective studies comparing cyclosporin monotherapy and methotrexate monotherapy for prevention of GVHD in patients receiving allogeneic BMT showed similar efficacy between treatment groups. In most studies, patients with haematological malignancies or aplastic anaemia received bone marrow matched at the major histocompatibility complex (human leucocyte antigen; HLA) from sibling donors.
In contemporary clinical practice, cyclosporin is the cornerstone of GVHD prophylaxis for patients receiving allogeneic BMT and is used concomitantly with other agents, usually methotrexate. In most noncomparative trials, prophylaxis with cyclosporin plus methotrexate was associated with an incidence of grade II to IV acute GVHD of approximately 30 to 40%. Probability of long term survival (2 to 6.8 years) ranged from 71 to 95% in patients with aplastic anaemia or other nonmalignant haematological disease and from 39 to 80% in studies in which most or all patients had haematological malignancies. Prospective randomised studies in patients with haematological malignancy or aplastic anaemia demonstrated that the combined use of cyclosporin plus methotrexate was more effective than either drug alone in preventing grade II to IV acute GVHD after BMT. Furthermore, the probability of survival tended to be or was statistically significantly increased in patients receiving combined therapy compared with those receiving cyclosporin or methotrexate monotherapy. In general, the severity of acute GVHD was also reduced with combined therapy compared with cyclosporin or methotrexate monotherapy.
Once established, GVHD is difficult to treat and cyclosporin has not been extensively evaluated in formal trials in this clinical setting. However, available data suggest that cyclosporin has similar efficacy to corticosteroids and that, whether used alone or in combination with corticosteroids, it is a useful treatment option for patients with acute GVHD.
Tolerability
Averse events associated with cyclosporin therapy for prevention of GVHD after BMT primarily involve the genitourinary system [renal dysfunction (60%)], gastrointestinal system [nausea or vomiting (40%) and diarrhoea (16%)], skin or mucous membranes [mucositis (30%) and rash (15%)] and CNS [tremor (23%)]. Oedema, hypertension, hypercholesterolaemia and a variety of other adverse events have also been reported.
Renal dysfunction is particularly common, but is generally reversible with cyclosporin dosage reduction, especially if nephrotoxicity develops during the first 6 months of therapy. Regular monitoring of serum creatinine levels is recommended as is therapeutic monitoring of drug concentrations, with cyclosporin dosage adjustments made as appropriate.
Cyclosporin has been shown to interact with a number of other drugs, resulting in increased nephrotoxicity, elevated or reduced serum/blood concentrations of cyclosporin or other effects depending on the interacting agent.
Dosage and Administration
For prevention of GVHD, cyclosporin is administered intravenously from the day prior to BMT at a dosage of 1.5 to 2.5 mg/kg every 12 hours until the patient is able to tolerate oral administration, usually after approximately 2 to 3 weeks. Thereafter, cyclosporin 5 to 6.25 mg/kg is given orally every 12 hours until day 50, after which the dosage is gradually reduced by 5% per week until discontinuation approximately 6 months after BMT. In some BMT centres, cyclosporin is administered orally from the onset (rather than intravenously for a short period initially) in selected patients.
For prevention of GVHD, the duration of prophylaxis with cyclosporin was 6 to 12 months after BMT in most clinical trials; however, some BMT centres use shorter courses of cyclosporin in patients with haematological malignancies in an effort to reduce relapse rates. Cyclosporin is typically used in combination with methotrexate for GVHD prophylaxis, although it is sometimes used in combination with corticosteroids or with both methotrexate and corticosteroids.
For treatment of patients with established grade II to IV acute GVHD, cyclosporin is administered orally at a dosage of 6.25 mg/kg every 12 hours or intravenously at a dosage of 2.5 mg/kg every 12 hours. Oral maintenance therapy should be continued until 6 months post-transplantation, after which dosage is gradually reduced and the drug is discontinued. A corticosteroid is frequently used in combination with cyclosporin for treating patients with established GVHD.
Similar content being viewed by others


References
Calne RY, White DJG, Thiru S, et al. Cyclosporin A in patients receiving renal allografts from cadaver donors. Lancet 1978; 2: 1323–7
Brodehl J. Consensus statements on the optimal use of cyclosporine in pediatric patients. Transplant Proc 1994 Oct; 26: 2759–62
Shaefer MS, Collier DS. Immunosuppression for solid organ transplantation. Dialysis Transplant 1993 Sep; 22: 542–53
Powles RL, Clink HM, Spence D, et al. Cyclosporin A to prvent graft-versus-host disease in man after allogeneic bone-marrow transplantation. Lancet 1980 Feb 16; 1: 327–9
Faulds D, Goa KL, Benfield P. Cyclosporin. A review of its pharmacodynamic and pharmacokinetic properties, and therapeutic use in immunoregulatory disorders. Drugs 1993 Jun; 45: 953–1040
Krensky AM, Clayberger C. Transplantation immunology. Pediatr Clin North Am 1994 Aug; 41: 819–39
Kahan BD. Immunosuppressive agents acting upon lymphokine synthesis and signal transduction. Clin Transpl 1993 Feb; 7 (Pt 2): 113–25
Kalechman Y, Sredni B, Caspi R, et al. Enhancing effect of cyclosporins A and G on bone marrow colony formation. Exp Hematol 1990 Nov; 18: 1104–7
Kosugi A, Shearer GM. Effect of cyclosporin A on lymphopoiesis. III. Augmentation of the generation of natural killer cells in bone marrow transplanted mice treated with cyclosporin A. J Immunol 1991 Mar 1; 146: 1416–21
Vannucchi AM, Bosi A, Grossi A, et al. Down-modulation of serum erythropoietin levels following cyclosporin A infusion [letter]. Bone Marrow Transplant 1994 Apr; 13: 497–8
Deeg HJ, Storb R, Weiden PL, et al. Cyclosporin A and methotrexate in canine marrow transplantation: engraftment, graft-versus-host disease, and induction of intolerance. Transplantation 1982 Jul; 34: 30–5
Denham S, Attridge S, Barfoot RK, et al. Effect of cyclosporin A on the anti-leukaemia action associated with graft-versus-host disease. Br J Cancer 1983 Jun; 47: 791–5
Horn TD, Bauer DJ, Vogelsang GB, et al. Reappraisal of histologic features of the acute cutaneous graft-versus-host reaction based on an allogeneic rodent model. J Invest Dermatol 1994 Aug; 103: 206–10
Markus PM, Cai X, Ming W, et al. Prevention of graft-versus-host disease following allogeneic bone marrow transplantation in rats using FK506. Transplantation 1991 Oct; 52: 590–4
Markwick JR, Chambers JD, Hobbs JR, et al. Timing of cyclosporin-A therapy for abrogation of HVG and GVH responses in rats. Lancet 1979 Nov 17; 2: 1037–40
van Bekkum DW, Knaan S, Zurcher C. Effects of cyclosporin A on experimental graft-versus-host disease in rodents. Transplant Proc 1980 Jun; 12: 278–82
van den Broek AA, Stet RJ, van Eden GG, et al. Graft versus host reaction in the rat: effect of cyclosporin A and cyclophosphamide on lymphocyte subsets involved in GVHR. Adv Exp Med Biol 1985; 186: 539–44
Cummins AG, Munro GH, Miller HR, et al. Effect of cyclosporin A treatment on the enteropathy of graft-versus-host reaction in the rat: a quantitative study of intestinal morphology, epithelial cell kinetics and mucosal immune activity. Immunol Cell Biol 1989 Jun; 67 (Pt 3): 153–60
Markus PM, Cai X, Ming W, et al. FK 506 reverses acute graft-versus-host disease after allogeneic bone marrow transplantation in rats. Surgery 1991 Aug; 110: 357–63 (discussion 363–4)
Rossi SJ, Schroeder TJ, Hariharan S. Prevention and management of the adverse effects associated with immunosuppressive therapy. Drug Saf 1993 Aug; 9: 104–31
Whiting PH. Acute and chronic nephrotoxicity associated with immunosuppressive drugs. Curr Opin Nephrol Hypertension 1994 Mar; 3: 174–81
dos Santos OF, Boim MA, Barros EJ, et al. Nephrotoxicity of cyclosporine: the role of platelet-activating factor and thromboxane. Lipids 1991; 26: 1320–3
Haug C, Duell T, Lenich A, et al. Elevated plasma endothelin concentrations in cyclosporin-treated patients after bone marrow transplantation. Bone Marrow Transplant 1995 July; 16: 191–4
Van Buren DH, Burke JF, Lewis RM. Renal function in patients receiving long-term cyclosporine therapy. J Am Soc Nephrol 1994 Feb; 4 Suppl. 1: S17–22
McEvoy GK, editor. AHFS Drug Information. Bethesda: American Society of Health-System Pharmacists, Inc., 1995
Butkus DE, Herrera GA, Raju SS. Successful renal transplantation after cyclosporine-associated hemolytic-uremic syndrome following bilateral lung transplantation. Transplantation 1992 July; 54(1): 159–62
Galli FC, Damon LE, Tomlanovich SJ, et al. Cyclosporine-induced hemolytic uremic syndrome in a heart transplant recipient. J Heart Lung Transplant 1993; 12: 440–4
Katznelson S, Wilkinson A, Rosenthal TR, et al. Cyclosporine-induced hemolytic uremic syndrome: factors that obscure its diagnosis. Transplant Proc 1994 October; 26(5): 2608–9
Fahr A. Cyclosporin clinical pharmacokinetics. Clin Pharmacokinet 1993 Jun; 24: 472–95
Yee GC. Pharmacokinetic and pharmacodynamic studies of cyclosporine in bone marrow transplantation. Transplant Proc 1990 Jun; 22: 1327–30
Gupta SK, Manfro RC, Tomlanovich SJ, et al. Effect of food on the pharmacokinetics of cyclosporine in healthy subjects following oral and intravenous administration. J Clin Pharmacol 1990; 30: 643–53
Schwinghammer TL, Przepiorka D, Venkataramanan R, et al. The kinetics of cyclosporine and its metabolites in bone marrow transplant patients. Br J Clin Pharmacol 1991 Sep; 32: 323–8
Lindholm A, Henricsson S, Lind M, et al. Intraindividual variability in the relative systemic availability of cyclosporin after oral dosing. Eur J Clin Pharmacol 1988; 34: 461–4
Noble S, Markham A. Cyclosporin. A review of the pharmacokinetic properties, clinical efficacy and tolerability of a microemulsion-based formulation (Neoral). Drugs 1995; 50(5): 924–41
Rodman JH, Stricklin L, Pederson A, et al. Cyclosporine clearance in pediatric patients undergoing bone marrow transplant using monoclonal whole blood assay [abstract]. Pharmacotherapy 1994 May–Jun; 14: 369
Yee GC, Kennedy MS, Storb R, et al. Effect of hepatic dysfunction on oral cyclosporin pharmacokinetics in marrow transplant patients. Blood 1984 Dec; 64: 1277–9
Yee GC, Mills G, Schaffer R, et al. Renal cyclosporine clearance in marrow transplant recipients: age-related variation. J Clin Pharmacol 1986 Nov–Dec; 26: 658–61
Krogh CME, editor. Compendium of Pharmaceuticals and Specialties. 30th edition, Ottawa: Canadian Pharmaceutical Association, 1995
Holt DW, Marwaha G, Jones K, et al. Quality assurance programs for immunosuppressive drugs: cyclosporine and beyond. Ther Drug Monit 1993 Dec; 15: 472–7
Atkinson K, Downs K, Ashby M, et al. Clinical correlations with cyclosporine blood levels after allogeneic bone marrow transplantation: an analysis of four different assays. Transplant Proc 1990 Jun; 22: 1331–4
Ghalie R, Fitzsimmons WE, Weinstein A, et al. Cyclosporine monitoring improves graft-versus-host disease prophylaxis after bone marrow transplantation. Ann Pharmacother 1994 Mar; 28: 379–83
Santos GW, Tutschka PJ, Brookmeyer R, et al. Cyclosporine plus methylprednisolone versus cyclophosphamide plus methyl-prednisolone as prophylaxis for graft-versus-host disease: a randomized double-blind study in patients undergoing allogeneic marrow transplantation. Clin Transpl 1987; 1: 21–8
Schmidt H, Einsele H, Jaschonek K, et al. Cyclosporine and graft-versus-host disease after bone marrow transplantation [letter]. N Engl J Med 1988 Dec 15; 319: 1607
Yee GC, Self SG, McGuire TR, et al. Serum cyclosporine concentration and risk of acute graft-versus-host disease after allogeneic marrow transplantation. N Engl J Med 1988 Jul 14; 319: 65–70
Kennedy MS, Yee GC, McGuire TR, et al. Correlation of serum cyclosporine concentration with renal dysfunction in marrow transplant recipients. Transplantation 1985 Sep; 40: 249–53
Brinch L, Evensen S, Albrechtsen D, et al. Fooled by blood cyclosporin levels [letter]. Bone Marrow Transplant 1992 Jan; 9: 77–8
Leson CL, Bryson SM, Giesbrecht EE, et al. Therapeutic monitoring of cyclosporine following pediatric bone marrow transplantation: problems with sampling from silicone central venous lines. DICP 1989 Apr; 23: 300–3
Soto J, Alsar MJ, Avendaño C, et al. Comparison of cyclosporine levels in samples obtained from central venous catheter with samples from peripheral sites in allogeneic bone marrow transplantation: implications in therapeutic monitoring of cyclosporine. Clin Transpl 1992 Oct; 6: 357–60
Lorenz RG, Garrett N, Turk JW, et al. Problems with therapeutic monitoring of cyclosporine using silicone central venous line samples [letter]. Transplantation 1991; 52: 1109–10
Deeg HJ, Henslee-Downey PJ. Management of acute graft-versus-host disease. Bone Marrow Transplant 1990 Jul; 6: 1–8
Parr MD, Messino MJ, Mclntyre W. Allogeneic bone marrow transplantation: procedures and complications. Am J Hosp Pharm 1991 Jan; 48: 127–37
Vogelsang GB, Morris LE. Prevention and management of graft-versus-host disease. Practical recommendations. Drugs 1993 May; 45: 668–76
Beatty PG, Hansen JA, Longton GM, et al. Marrow transplantation from HLA-matched unrelated donors for treatment of hematologic malignancies. Transplantation 1991; 51: 443–7
McGlave P, Bartsch G, Anasetti C, et al. Unrelated donor marrow transplantation for chronic myelogenous leukemia: initial experience of the national marrow donor program. Blood 1993; 81: 543–50
Thomas ED, Storb R, Clift RA, et al. Bone marrow transplantation (second of two parts). N Engl J Med 1975; 292(17): 895–902
Wick MR, Moore SB, Gastineau DA, et al. Immunologic, clinical and pathologic aspects of human graft-versus-host disease. Mayo Clin Proc 1983; 58: 603–12
Ringdén O. Management of graft-versus-host disease. Eur J Haematol 1993 Jul; 51: 1–12
Wagner JE, Vogelsang GB, Beschorner WE. Pathogenesis and pathology of graft-versus-host disease. Am J Pediatr Hematol Oncol 1989; 11: 196–212
Crawford SW, Clark JG. Bronchiolitis associated with bone marrow transplantation. Clin Chest Med 1993 Dec; 14: 741–9
Schwinghammer TL, Bloom EJ. Pharmacologic prophylaxis of acute graft-versus-host disease after allogeneic marrow transplantation. Clin Pharm 1993 Oct; 12: 736–61
Gratwohl A, Tichelli A, Nissen C, et al. Treatment of GVHD with cyclosporin A. Bone Marrow Transplant 1993; 12 Suppl. 3: 32–5
Tsoi M-S, Storb R, Dobbs S, et al. Specific suppressor cells in graft-host tolerance of HLA-identical marrow transplant patients. Blood 1981; 64: 215–20
Hess AD, Jones RJ, Morris LE, et al. Autologous graft-versus-host disease: a novel approach for antitumor immunotherapy. Hum Immunol 1992 Jul; 34: 219–24
Sosman JA, Sondel PM. The graft-vs.-leukemia effect. Implications for post-marrow transplant antileukemia treatment. Am J Pediatr Hematol Oncol 1993 May; 15: 185–95
Kennedy MJ. Induction of graft-versus-host syndrome as a treatment for breast cancer. Clin Immunother 1994 Mar; 1: 173–80
Kennedy MJ. Induced autologous graft-versus-host disease for the treatment of cancer. Cancer Treat Rev 1994 Jan; 20: 97–103
Carella AM, Gaozza E, Congiu A, et al. Cyclosporine-induced graft-versus-host disease after autologous bone marrow transplantation in hematological malignancies. Ann Hematol 1991 May; 62: 156–9
Dale BM, Atkinson K, Kotasek D, et al. Cyclosporine-induced graft vs host disease in two patients receiving syngeneic bone marrow transplants. Transplant Proc 1989 Oct; 17: 3816–7
Jones RJ, Vogelsang GB, Hess AD, et al. Induction of graft-versus-host disease after autologous bone marrow transplantation. Lancet 1989 Apr 8; 1: 754–7
Kennedy MJ, Vogelsang GB, Beveridge RA, et al. Phase I trial of intravenous cyclosporine to induce graft-versus-host disease in women undergoing autologous bone marrow transplantation for breast cancer. J Clin Oncol 1993 Mar; 11: 478–84
Rizzoli V, Carella AM, Carlo-Stella C, et al. Autologous marrow transplantation in acute lymphoblastic leukemia: control of residual disease with mafosfamide and induction of syngeneic GVHD with cyclosporin. Bone Marrow Transplant 1990 Jul; 6 Suppl. 1: 76–8
Talbot DC, Powles RL, Sloane JP, et al. Cyclosporine-induced graft-versus-host disease following autologous bone marrow transplantation in acute myeloid leukaemia. Bone Marrow Transplant 1990 Jul; 6: 17–20
Yeager AM, Vogelsang GB, Jones RJ, et al. Cyclosporine-induced graft-versus-host disease after autologous bone marrow transplantation for acute myeloid leukemia. Leuk Lymphoma 1993 Oct; 11: 215–20
Barrett AJ, Kendra JR, Lucas CF, et al. Cyclosporin A as prophylaxis against graft-versus-host disease in 36 patients. Br Med J Clin Res Ed 1982 Jul 17; 285: 162–6
Champlin R, Ho W, Gajewski J, et al. Selective depletion of CD8+ T lymphocytes for prevention of graft-versus-host disease after allogeneic bone marrow transplantation. Blood 1990 Jul 15; 76: 418–23
Gluckman E, Arcese W, Devergie A, et al. Cyclosporin-A prophylactic treatment of graft-versus-host disease in human allogeneic bone marrow transplantation: preliminary results. Transplant Proc 1981 Mar; 13(1): 368–70
Gratwohl A, Speck B, Wenk M, et al. Cyclosporine in human bone marrow transplantation. Serum concentration, graft-versus-host disease, and nephrotoxicity. Transplantation 1983 Jul; 36: 40–4
Harper JI, Kendra JR, Desai S, et al. Dermatological aspects of the use of Cyclosporin A for prophylaxis of graft-versus-host disease. Br J Dermatol 1984 Apr; 110: 469–74
Ruutu T, Volin L, Elonen E. Low incidence of severe acute and chronic graft-versus-host disease as a result of prolonged cyclosporine prophylaxis and early aggressive treatment with corticosteroids. Transplant Proc 1988 Jun; 20: 491–3
Sullivan KM, Deeg HJ, Sanders J, et al. Hyperacute graft-v-host disease in patients not given immunosuppression after allogeneic marrow transplantation. Blood 1986 Apr; 67: 1172–5
Tutschka PJ, Hess AD, Beschorner WE, et al. Cyclosproine in clinical marrow transplantation: the Baltimore experience. Transplant Proc 1983; 15(4): 2613–6
Bacigalupo A, Van Lint MT, Occhini D, et al. Increased risk of leukemia relapse with high-dose cyclosporine A after allogeneic marrow transplantation for acute leukemia. Blood 1991 Apr 1; 77: 1423–8
Fagioli F, Bacigalupo A, Frassoni F, et al. Allogeneic bone marrow transplantation for acute myeloid leukemia in first complete remission: the effect of FAB classification and GVHD prophylaxis. Bone Marrow Transplant 1994 Mar; 13: 247–52
Bacigalupo A, Maiolino A, Van Lint MT, et al. Cyclosporin-A and chronic graft versus host disease. Bone Marrow Transplant 1990 Nov; 6: 341–4
Locatelli F, Uderzo C, Dini G, et al. Graft-versus-host disease in children: the AIEOP-BMT Group experience with cyclosporin A. Bone Marrow Transplant 1993 Dec; 12: 627–33
Biggs JC, Atkinson K, Gillett E, et al. A randomized prospective trial comparing cyclosporine and methotrexate given for prophylaxis of graft-versus-host disease after bone marrow transplantation. Transplant Proc 1986 Apr; 18: 253–5
Deeg HJ, Storb R, Thomas ED, et al. Marrow transplantation for acute nonlympholblastic leukemia in first remission: preliminary results of a randomized trial comparing cyclosporine and methotrexate for the prophylaxis of graft-versus-host disease. Transplant Proc 1983; 15(1): 1385–8
Deeg HJ, Storb R, Thomas ED, et al. Cyclosporine as prophylaxis for graft-versus-host disease: a randomized study in patients undergoing marrow transplantation for acute nonlymphoblastic leukemia. Blood 1985 Jun; 65: 1325–34
Irle C, Deeg HJ, Buckner CD, et al. Marrow transplantation for leukemia following fractionated total body irradiation. A comparative trial of methotrexate and cyclosporine. Leuk Res 1985; 9: 1255–61
Ringdén O, Bäckman L, LÖnnqvist B, et al. A randomized trial comparing use of cyclosporin and methotrexate for graft-versus-host disease prophylaxis in bone marrow transplant recipients with haematological malignancies. Bone Marrow Transplant 1986 May; 1: 41–51
Storb R, Deeg HJ, Thomas ED, et al. Marrow transplantation for chronic myelocytic leukemia: a controlled trial of cyclosporine versus methotrexate for prophylaxis of graft-versus-host disease. Blood 1985 Sep; 66: 698–702
Torres A, Martinez F, Gomez P, et al. Cyclosporin A versus methotrexate, followed by rescue with folinic acid as prophylaxis of acute graft-versus-host disease after bone marrow transplantation. Blut 1989 Feb; 58: 63–8
Storb R, Deeg HJ, Fisher L, et al. Cyclosporine v methotrexate for graft-v-host disease prevention in patients given marrow grafts for leukemia: long-term follow-up of three controlled trials. Blood 1988 Feb; 71: 293–8
Storb R, Deeg HJ, Pepe M, et al. Long-term follow-up of three controlled trials comparing cyclosporine versus methotrexate for graft-versus-host disease prevention in patients given marrow grafts for leukemia. Blood 1992 Jun 1; 79: 3091–2
Atkinson K, Biggs JC, Concannon A, et al. A prospective randomised trial of cyclosporin versus methotrexate after HLA-identical sibling marrow transplantation for patients with acute leukemia in first remission: analysis 2.5 years after last patient entry. Aust N Z J Med 1988 Jun; 18: 594–9
Bäckman L, Ringdén O, Tollemar J, et al. An increased risk of relapse in cyclosporin-treated compared with methotrexate-treated patients: long-term follow-up of a randomized trial. Bone Marrow Transplant 1988 Sep; 3: 463–71
Horowitz MM, Gale RP, Barrett AJ, et al. Effect of methotrexate on relapse after bone marrow transplantation for acute lymphoblastic leukaemia. Lancet 1989; 1: 535–7
Weiner RS, Bortin MM, Gale RP, et al. Interstitial pneumonitis after bone marrow transplantation. Assessment of risk factors. Ann Intern Med 1986 Feb; 104: 168–75
Weiner RS, Horowitz MM, Gale RP, et al. Risk factors for interstitial pneumonia following bone marrow transplantation for severe aplastic anaemia. Br J Haematol 1989 Apr; 71: 535–43
Bortin MM, Horowitz MM, Rowlings PA, et al. 1993 progress report from the International Bone Marrow Transplant Registry. Bone Marrow Transplant 1993 Aug; 12: 97–104
Gale RP, Bortin MM, van-Bekkum DW, et al. Risk factors for acute graft-versus-host disease. Br J Haematol 1987 Dec; 67: 397–406
Angelucci E, Baronciani D, Lucarelli G, et al. Bone marrow transplantation in class 3 thalassaemia patients. Bone Marrow Transplant 1993; 12 Suppl. 1: 63–4
Arranz R, Otero MJ, Ramos R, et al. Clinical results in 50 multiply transfused patients with severe aplastic anemia treated with bone marrow transplantation or immunosuppressive therapy. Bone Marrow Transplant 1994 Apr; 13: 383–7
Beelen DW, Quabeck K, Kaiser B, et al. Six weeks of continuous intravenous cyclosporine and short-course methotrexate as prophylaxis for acute graft-versus-host disease after allogeneic bone marrow tranplantation. Transplantation 1990 Sep; 50: 421–7
Chiu EKW, Hawkins BR, Liang RHS, et al. Incidence of graft-versus-host disease in Hong Kong Chinese and its influence on survival after bone marrow transplantation from HLA-identical siblings. Bone Marrow Transplant 1995 April; 15: 543–7
Deeg HJ, Spitzer TR, Cottier-Fox M, et al. Conditioning-related toxicity and acute graft-versus-host disease in patients given methotrexate/cyclosporine prophylaxis. Bone Marrow Transplant 1991 Mar; 7: 193–8
Galimberti M, Polchi P, Lucarelli G, et al. Allogeneic marrow transplantation in patients with chronic myeloid leukemia in chronic phase following preparation with busulfan and cyclophosphamide. Bone Marrow Transplant 1994 Feb; 13: 197–201
Hashino S, Imamura M, Kasai M, et al. Bone marrow transplantation for hematological diseases in Hokkaido — June 1985 to December 1991. Jpn J Clin Oncol 1993 Jun; 23: 166–72
Hunter AE, Bessell EM, Russell NH. Effective prevention of acute GVHD following allogeneic BMT with low leukaemic relapse using methotrexate and therepeutically monitored levels of cyclosporin A. Bone Marrow Transplant 1992 Nov; 10: 431–4
Marks DI, Cullis JO, Ward KN, et al. Allogeneic bone marrow transplantation for chronic myeloid leukemia using sibling and volunteer unrelated donors. A comparison of complications in the first 2 years. Ann Intern Med 1993 Aug 1; 119: 207–14
Miller KB, Schenkein DP, Erban JK, et al. Adjusted dose continuous-infusion cyclosporin A to prevent graft-versus-host disease following allogeneic bone marrow transplantation. Ann Hematol 1994 Jan; 68: 15–20
Nash RA, Pepe MS, Storb R, et al. Acute graft-versus-host disease: analysis of risk factors after allogeneic marrow transplantation and prophylaxis with cyclosporine and methotrexate. Blood 1992 Oct 1; 80: 1838–45
Russell JA, Woodman RC, Poon M-C, et al. Addition of low-dose folinic acid to a methotrexate/cyclosporin A regimen for prevention of acute graft-versus-host disease. Bone Marrow Transplant 1994 Sep; 14: 397–401
Storb R, Sanders JE, Pepe M, et al. Graft-versus-host disease prophylaxis with methotrexate/cyclosporine in children with severe aplastic anemia treated with cyclophosphamide and HLA-identical marrow grafts [letter]. Blood 1991 Aug 15; 78: 1144–5
von Bueltzingsloewen A, Belanger R, Perreault C, et al. Acute graft-versus-host disease prophylaxis with methotrexate and cyclosporine after busulfan and cyclophosphamide in patients with hematologic malignancies. Blood 1993 Feb 1; 81: 849–55
Storb R, Deeg HJ, Whitehead J, et al. Methotrexate and cyclosporine compared with cyclosporine alone for prophylaxis of acute graft versus host disease after marrow transplantation for leukemia. N Engl J Med 1986 Mar 20; 314: 729–35
Nademanee A, Schmidt GM, Parker P, et al. The outcome of matched and unrelated donor bone marrow transplantation in patients with hematologic malignancies using molecular typing for donor selection and graft-versus-host disease prophylaxis regimen of cyclosporine, methotrexate, and prednisone. Blood 1995 August 1; 86: 1228–34
Bullorsky EO, Puppo MI, Shanley CM, et al. Ciclosproine A (CsA) and prednisone (pred) protocol for the prophylaxis of acute graft versus host disease (AGvHD) [abstract no. 2804]. Blood 1994 November 15; 84(10) Suppl. 1: 705a
Schwinghammer TL, Bloom EJ, Rosenfeld CS, et al. High-dose cyclosporine and corticosteroids for prophylaxis of acute chronic graft-versus-host-disease. Bone Marrow Transplant 1995; 16: 147–54
Shepherd JD, Shore TB, Reece D, et al. Cyclosporine and methylprednisolone for prophylaxis of acute graft-versus-host disease. Bone Marrow Transplant 1988; 3: 553–8
Jansen J, Hanks S, Akard L, et al. Selective T cell depletion with CD8-conjugated magnetic beads in the prevention of graft-versus-host disease after allogeneic bone marrow transplantation. Leukemia 1995; 9: 271–8
Drobyski WR, Ash RC, Casper JT, et al. Effect of T-cell depletion as graft-versus-host disease prophylaxis on engraftment, relapse, and disease-free survival in unrelated marrow transplantation for chronic myelogenous leukemia. Blood 1994 Apr 1; 83: 1980–7
Atkinson K, Biggs J, Concannon A, et al. A prospective randomised trial of cyclosporin and methotrexate versus cyclosporin, methotrexate and prednisolone for prevention of graft-versus-host disease after HLA-identical sibling marrow transplantation for haematological malignancy. Aust NZ J Med 1991 Dec; 21: 850–6
Mrsic M, Labar B, Bogdanic V, et al. Combination of cyclosporin and methotrexate for prophylaxis of acute graft-versus-host disease after allogeneic bone marrow transplantation for leukemia. Bone Marrow Transplant 1990 Aug; 6: 137–41
Ringdén O, Pihlstedt P, Markling L, et al. Prevention of graft-versus host disease with T cell depletion or cyclosporin and methotrexate. A randomized trial in adult leukemic marrow recipients. Bone Marrow Transplant 1991 Mar; 7: 221–6
Storb R, Deeg HJ, Farewell V, et al. Marrow transplantation for severe aplastic anemia: methotrexate alone compared with a combination of methotrexate and cyclosporine for prevention of acute graft-versus-host disease. Blood 1986 Jul; 68: 119–25
Storb R, Pepe M, Anasetti C, et al. What role for prednisone in prevention of acute graft-versus-host-disease in patients undergoing marrow transplants? Blood 1990 Sep 1; 76: 1037–45
Chao NJ, Schmidt GM, Niland JC, et al. Cyclosporine, methotrexate, and prednisone compared with cyclosporine and prednisone for prophylaxis of acute graft-versus-host disease. N Engl J Med 1993 Oct 21; 329: 1225–30
Galimberti M, Polchi P, Lucarelli G, et al. A comparative trial of posttransplant immunosuppression in patients transplanted for thalassemia. Cyclosporine alone versus cyclosporine, cyclophosphamide, and methotrexate. Transplantation 1988 Mar; 45: 566–9
Forman SJ, Blume KG, Krance RA, et al. A prospective randomized study of acute graft-vs-host disease in 107 patients with leukemia: methotrexate/prednisone vs cyclosporine/prednisone. Transplant Proc 1987; 19: 2605–7
Storb R, Pepe M, Deeg HJ, et al. Long-term follow-up of a controlled trial comparing a combination of methotrexate plus cyclosporine with cyclosporine alone for prophylaxis of graft-versus-host disease in patients administered HLA-identical marrow grafts for leukemia. Blood 1992 Jul 15; 80: 560
Storb R, Deeg HJ, Pepe M, et al. Graft-versus-host disease prevention by methotrexate combined with cyclosporin compared to methotrexate alone in patients given marrow grafts for severe aplastic anaemia: long-term follow-up of a controlled trial [see comments]. Br J Haematol 1989 Aug; 72: 567–72
Storb R, Leisenring W, Deeg HJ, et al. Long-term follow-up of a randomized trial of graft-versus-host disease prevention by methotrexate/cyclosporine versus methotrexate alone in patients given marrow grafts for severe aplastic anemia. Blood 1994 May 1; 83: 2749–50
Aschan J, Ringden O, Sundberg B, et al. Methotrexate combined with cyclosporin A decreases graft-versus-host disease, but increases leukemic relapse compared to monotherapy. Bone Marrow Transplant 1991 Feb; 7: 113–9
Aschan J, Ringdén O, Sundberg B, et al. Increased risk of relapse in patients with chronic myelogenous leukemia given T-cell depleted marrow compared to methotrexate combined with cyclosporin or monotherapy for the prevention of graft-versus-host disease. Eur J Haematol 1993 May; 50: 269–74
Aschan J, Ringdén O. Prognostic factors for long-term survival in leukemic marrow recipients with special emphasis on age and prophylaxis for graft-versus-host disease. Clin Transpl 1994 Jun; 8 (Pt 1): 258–70
Atkinson K, Biggs JC, Concannon AJ, et al. Changing results of HLA-identical sibling bone marrow transplantation in patients with haematological malignancy during the period 1981–1990. Aust N Z J Med 1993 Apr; 23: 181–6
Gluckman E, Devergie A, Lokiec F. Use of cyclosporine for prevention of graft-versus-host disease after allogeneic bone marrow transplantation. Transplant Proc 1988 Jun; 20(3) Suppl. 3: 461–9
Gratama JW, v.d. Nat H, Weiland HT, et al. Intensification of GVHD prophylaxis interferes with the effects of pretransplant herpes virus serology on the occurrence of grades II-IV acute graft-versus-host disease. Ann Hematol 1992 Jun; 64 Suppl.: A137–9
Hägglund H, Boström L, Ringdén O, et al. Risk factors for acute graft-versus-host disease in 325 consecutive bone marrow recipients. Transplant Proc 1994 Jun; 26: 1821–2
Marks DI, Hughes TP, Szydlo R, et al. HLA-identical sibling donor bone marrow transplantation for chronic myeloid leukaemia in first chronic phase: influence of GVHD prophylaxis on outcome. Br J Haematol 1992 Jul; 81: 383–90
Martin PJ, Schoch G, Fisher L, et al. A retrospective analysis of therapy for acute graft-versus-host disease: initial treatment. Blood 1990 Oct 15; 76: 1464–72
Michallet M, Corront B, Bosson JL, et al. Role of splenectomy in incidence and severity of acute graft-versus-host disease: a multicenter study of 157 patients. Bone Marrow Transplant 1991 Jul; 8: 13–7
Ringdén O, Klaesson S, Sundberg B, et al. Decreased incidence of graft-versus-host disease and improved survival with methotrexate combined with cyclosporin compared with monotherapy in recipients of bone marrow from donors other than HLA identical siblings. Bone Marrow Transplant 1992 Jan; 9: 19–25
Ringdén O, Horowitz MM, Sondel P, et al. Methotrexate, cyclosporine, or both to prevent graft-versus-host disease after HLA-identical sibling bone marrow transplants for early leukemia? Blood 1993 Feb 15; 81: 1094–101
Ringdén O. Decreased transplant-related complications and improved leukemia-free survival in adults receiving methotrexate combined with cyclosporin compared with either agent alone for prevention of graft-versus-host disease. Transplant Proc 1993 Feb; 25 (Part 2): 1241–2
Sanders JE, Storb R, Anasetti C, et al. Marrow transplant experience for children with severe aplastic anemia. Am J Pediatr Hematol Oncol 1994 Feb; 16: 43–9
Tollemar J, Ringdén O, Sundberg B, et al. Decreased incidence of graft-versus-host disease in bone marrow transplantation recipients treated with a combination of cyclosporine and methotrexate. Transplant Proc 1988 Jun; 20: 494–8
Vogler WR, Winton EF, Reynolds RC, et al. Factors affecting survival in allogeneic bone marrow transplantation. Am J Med Sci 1989 May; 297: 300–8
Gluckman E, Horowitz MM, Champlin RE, et al. Bone marrow transplantation for severe aplastic anemia: influence of conditioning and graft-versus-host disease prophylaxis regimens on outcome. Blood 1992 Jan 1; 79: 269–75
Nevill TJ, Tirgan MH, Deeg HJ, et al. Influence of post-methotrexate folinic acid rescue on regimen-related toxicity and graft-versus-host disease after allogeneic bone marrow transplantation. Bone Marrow Transplant 1992 May; 9: 349–54
Nimer SD, Giorgi J, Gajewski JL, et al. Selective depletion of CD8+ cells for prevention of graft-versus-host disease after bone marrow transplantation. A randomized controlled trial. Transplantation 1994 Jan; 57: 82–7
Hale G, Waldmann H. Control of graft-versus-host disease and graft rejection by T cell depletion of donor and recipient with Campath-1 antibodies. Results of matched sibling transplants for malignant diseases. Bone Marrow Transplant 1994 May; 13: 597–611
Bunjes D, Hertenstein B, Wiesneth M, et al. In vivo/ex vivo T cell depletion reduces the morbidity of allogeneic bone marrow transplantation in patients with acute leukaemias in first remission without increasing the risk of treatment failure: comparison with cyclosporin/methotrexate. Bone Marrow Transplant 1995 April; 15: 563–8
Blaise D, Olive D, Michallet M, et al. Impairment of leukaemia-free survival by addition of interleukin-2-receptor antibody to standard graft-versus-host prophylaxis. Lancet 1995 May 6; 345: 1144–6
Leelasiri A, Greer JP, Stein RS, et al. Graft-versus-host-disease prophylaxis for matched unrelated donor bone marrow transplantation: comparison between cyclosporine-methotrexate and cyclosporine-methotrexate-methylprednisolone. Bone Marrow Transplant 1995; 15: 401–5
Aschan J. Treatment of moderate to severe acute graft-versus-host disease: a retrospective analysis. Bone Marrow Transplant 1994 Oct; 14: 601–7
Martin PJ, Schoch G, Fisher L, et al. A retrospective analysis of therapy for acute graft-versus-host disease: secondary treatment. Blood 1991 Apr 15; 77: 1821–8
Kennedy MS, Deeg HJ, Storb R, et al. Treatment of acute graft-versus-host disease after allogeneic marrow transplantation. Randomized study comparing corticosteroids and cyclosporine. Am J Med 1985 Jun; 78 (6 Pt 1): 978–83
Bunjes D, Heit W, Arnold R, et al. Cyclosporine as an alternative to cyclophosphamide in the treatment of chronic graft-versus-host disease. Transplantation 1986 Feb; 41: 170–2
Deeg HJ, Loughran Jr TP, Storb R, et al. Treatment of human acute graft-versus-host disease with antithymocyte globulin and cyclosporine with or without methylprednisolone. Transplantation 1985 Aug; 40: 162–6
Epstein JB, Reece DE. Topical cyclosporin A for treatment of oral chronic graft-versus-host disease. Bone Marrow Transplant 1994 Jan; 13: 81–6
Powles RL, Barrett AJ, Clink H, et al. Cyclosporin A for the treatment of graft-versus-host disease in man. Lancet 1978 Dec 23–30; 2: 1327–31
Sanchez MA, Bacot BK, Hanson IC, et al. Bolus methylprednisolone with cyclosporine (CSA) treatment of chronic gastrointestinal graft-versus-host disease (GI GVHD) after allogeneic bone marrow transplant (BMT). J Allergy Clin Immunol 1994 Jan; 93 (Pt 2): 204
Sullivan KM, Witherspoon RP, Storb R, et al. Alternating-day cyclosporine and prednisone for treatment of high-risk chronic graft-v-host disease. Blood 1988 Aug; 72: 555–61
Yasukawa M, Shinozaki F, Hato T, et al. Successful treatment of transfusion-associated graft-versus-host disease. Br J Haematol 1994 Apr; 86: 831–6
Yee GC, McGuire TR, St Pierre BA, et al. Minimal risk of chronic renal dysfunction in marrow transplant recipients treated with cyclosporine for 6 months. Bone Marrow Transplant 1989 Nov; 4: 691–4
Loughran Jr TP, Deeg HJ, Dahlberg S, et al. Incidence of hypertension after marrow transplantation among 112 patients randomized to either cyclosporine or methotrexate as graft-versus-host disease prophylaxis. Br J Haematol 1985 Mar; 59: 547–53
Avery R, Jabs DA, Wingard JR, et al. Optic disc edema after bone marrow transplantation. Possible role of cyclosporine toxicity. Ophthalmology 1991 Aug; 98: 1294–301
Fiorani L, Bandini G, D’Alessandro R, et al. Cyclosporin A neurotoxicity after allogeneic bone marrow transplantation. Bone Marrow Transplant 1994 Jul; 14: 175–6
Reece DE, Frei-Lahr DA, Shepherd JD, et al. Neurologic complications in allogeneic bone marrow transplant patients receiving cyclosporin. Bone Marrow Transplant 1991 Nov; 8: 393–401
De Klippel N, Sennesael J, Lamote J, et al. Cyclosporin leukoencephalopathy induced by intravenous lipid solution [letter]. Lancet 1992 May 2; 339: 114
Shimizu C, Kimura S, Yoshida Y, et al. Acute leucoencephalopathy during cyclosporin A therapy in a patient with nephrotic syndrome. Pediatr Nephrol 1994; 8: 483–5
Memon M, deMagalhaes-Silverman M, Bloom EJ, et al. Reversible cyclosporine-induced cortical blindness in allogeneic bone marrow transplant recipients. Bone Marrow Transplant 1995; 15: 283–6
Lopez-Miranda J, Pérez-Jimenéz F, Torres A, et al. Effect of cyclosporin on plasma lipoproteins in bone marrow transplantation patients. Clin Biochem 1992 Oct; 25: 379–86
Luke DR, Beck JE, Vadiei K, et al. Longitudinal study of cyclosporine and lipids in patients undergoing bone marrow transplantation. J Clin Pharmacol 1990 Feb; 30: 163–9
Bulengo-Ransby SM, Sahn EE, Metcalf JS, et al. Bowenoid change in association with graft-versus-host disease: a cyclosporine toxicity? J Am Acad Dermatol 1994 Dec; 31: 1052–4
Palou J, Martin E, Mascaro JM, et al. Cyclosporin A and graft-vs.-host disease [letter]. Am J Dermatopathol 1986 Feb; 8: 90–1
Hatta Y, Tomura K, Kawamura M, et al. Microangiopathic hemolytic anemia in a graft-versus-host disease patient treated with cyclosporine A and prednisolone. Intern Med 1992 Mar; 31: 434–7
Holler E, Kolb HJ, Hiller E, et al. Microangiopathy in patients on cyclosporine prophylaxis who developed acute graft-versus-host disease after HLA-identical bone marrow transplantation. Blood 1989 May 15; 73: 2018–24
Pettitt AR, Clark RE. Thrombotic microangiopathy following bone marrow transplantation. Bone Marrow Transplant 1994 Oct; 14: 495–504
Horton RC, Bonser RS. Interaction between cyclosporin and fluoxetine. BMJ 1995 August 12; 311: 422
Gilbert RD, Kahn D, Cassidy M. Interaction between clonidine and cyclosporin A. Nephron 1995 September; 71: 105
Anonymous. National Cholesterol Education Program: second report of the expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (adult treatment panel II). Circulation 1994; 89: 1333–445
Huang LQ, Whitworth JA, Chesterman CN. Effects of cyclosporin A and dexamethasone on haemostatic and vasoactive functions of vascular endothelial cells. Blood Coagul Fibrinolysis 1995; 6: 438–45
Monsour Jr HP, Wood RP, Dyer CH, et al. Renal insufficiency and hypertension as long-term complications in liver transplantation. Semin Liver Dis 1995; 15(2): 123–32
Pirsch JD, Armbrust JM, Knechtle SJ, et al. Effect of steroid withdrawal on hypertension and cholesterol levels in living related recipients. Transplant Proc 1991; 23(1): 1363–4
Christophidis N, Ryan P, Angelis P, et al. Grapefruit juice and cyclosporin A blood concentrations in patients with rheumatic diseases [abstract]. Aust N Z J Med 1995; 25(4): 388
Ducharme MP, Warbasse LH, Edwards DJ. Disposition of intravenous and oral cyclosproine after administration with grapefruit juice. Clin Pharmacol Ther 1995 May; 57(5): 485–91
Hollander AAMJ, van Rooij J, Lentjes EGWM, et al. The effect of grapefruit juice on cyclosporine and prednisone metabolism in transplant patients. Clin Pharmacol Ther 1995; 57: 318–24
Proppe DG, Hoch OD, McLean AJ, et al. Influence of chronic ingestion of grapefruit juice on steady-state blood concentrations of cyclosporine A in renal transplant patients with stable graft function [letter]. Br J Clin Pharmacol 1995; 39: 337
Yee GC, Stanley DL, Pessa LJ, et al. Effect of grapefruit juice on blood cyclosporin concentration. Lancet 1995; 345: 955–6
D’Arcy PF. Effect of grapefruit juice on blood cyclosporin concentrations. Int Pharm J 1995; 9(4): 142–3
Liesveld JL, Packman CH, Abboud CN, et al. Use of GVHD prophylaxis with continuous infusion cyclosporin A, nifedipine, methotrexate, and steroids in matched unrelated donor transplants (MUDS) [abstract no. 1351]. Blood 1994 Nov 15; 84(10) Suppl. 1: 341a
Phillips GL, Nevill TJ, Spinelli JJ, et al. Prophylaxis for acute graft-versus-host disease following unrelated donor bone marrow transplantation. Bone Marrow Transplant 1995; 15: 213–9
Author information
Authors and Affiliations
Additional information
Various sections of the manuscript reviewed by: J. Aschan, Department of Clinical Immunology, Huddinge Hospital, Huddinge, Sweden; A. Bacigalupo, Department of Hematology, Ospedale San Martino, Genova, Italy; N.J. Chao, Division of Bone Marrow Transplantation, Department of Medicine, Stanford University School of Medicine, Stanford University Medical Center, Stanford, California, USA; A.E. Hunter, Department of Haematology, Nottingham City Hospital, Nottingham, England; J.H. Lipton, Bone Marrow Transplant Program, Ontario Cancer Institute, Princess Margaret Hospital, Toronto, Ontario, Canada; R.A. Nash, Clinical Research Division, Transplantation Biology Department, Fred Hutchinson Cancer Research Center, Seattle, Washington, USA; O. Ringdén, Division of Clinical Immunology, Department of Immunology, Microbiology, Pathology and Infectious Diseases, Huddinge University Hospital, Huddinge, Sweden; J.A. Russell, Alberta Bone Marrow Transplant Program, Tom Baker Cancer Centre, Southern Alberta Cancer Program, Calgary, Alberta, Canada; G.B. Vogelsang, Johns Hopkins Bone Marrow Transplant Unit, Johns Hopkins Hospital, Baltimore, Maryland, USA; M. Yasukawa, First Department of Internal Medicine, Ehime University School of Medicine, Shigenobu, Ehime, Japan.
Rights and permissions
About this article
Cite this article
Plosker, G.L., Barradell, L.B. Cyclosporin. Clin Immunother 5, 59–90 (1996). https://doi.org/10.1007/BF03259315
Published:
Issue Date:
DOI: https://doi.org/10.1007/BF03259315