
Abstract
Background: Most patients with hypertension will require combination therapy with at least two agents from different antihypertensive classes to achieve blood pressure (BP) control. Thiazide diuretics, such as hydrochlorothiazide (HCTZ), are widely used in combination therapy. The volume reduction with these agents stimulates the renin-angiotensin system (RAS), making RAS inhibitors such as the direct renin inhibitor aliskiren a logical choice for combination therapy with HCTZ.
Objective: The aim of this study was to investigate the long-term safety, tolerability and efficacy of the direct renin inhibitor aliskiren, with or without addition of the diuretic HCTZ.
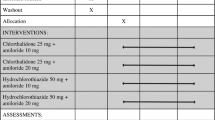
Methods: In the 12-month core study, patients with hypertension (mean sitting diastolic BP ≥90 mmHg and <110 mmHg) were randomized in a 3:2 ratio to once-daily aliskiren 150 mg or 300 mg. At months 2, 3,4, 6 and 9, treatment was adjusted in patients not achieving a BP goal of <140/90mmHg. Patients not at goal on aliskiren 150 mg once daily were up-titrated to aliskiren 300 mg once daily. Patients not at goal with aliskiren 300 mg once daily received addon HCTZ 12.5 mg once daily, which was up-titrated to 25 mg once daily if BP remained inadequately controlled. At month 12, patients who received aliskiren/HCTZ 300 mg/25 mg once daily for at least 8 months in the core study were eligible to enter a 4-month extension study.
Results: Overall, 1625/1955 patients completed the core study, and 870/1955 patients received add-on HCTZ; 189/198 patients completed the 4-month extension. Aliskiren, with or without add-on HCTZ, was generally well tolerated; the incidence of adverse events (AEs) during the core study was similar among the four final treatment groups. The most frequently reported AEs in the core and extension studies were mild and transient cases of nasopharyngitis, headache and dizziness. Few patients exhibited laboratory abnormalities. Overall, aliskiren, with or without add-on HCTZ, reduced mean BP by 18.0/12.7mmHg at core study endpoint, and 61.2% of patients achieved BP control. BP reductions with aliskiren/HCTZ 300 mg/25 mg combination therapy at the core study endpoint were maintained during the extension study.
Conclusion: In patients with hypertension, long-term treatment with aliskiren, with or without add-on HCTZ, is well tolerated and provides effective BP lowering that is sustained over 12 months.
Trial Registration: ClinicalTrials.gov Identifier NCT00219037.









Similar content being viewed by others


References
Chobanian AV, Bakris GL, Black HR, et al. Seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Hypertension 2003; 42: 1206–52
Mancia G, De Backer G, Dominiczak A, et al. 2007 Guidelines for the management of arterial hypertension: The Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). J Hypertens 2007; 25: 1105–87
Waeber B. Combination therapy with ACE inhibitors/ angiotensin II receptor antagonists and diuretics in hypertension. Expert Rev Cardiovasc Ther 2003; 1: 43–50
Frampton JE, Curran MP. Aliskiren: a review of its use in the management of hypertension. Drugs 2007; 67: 1767–92
Villamil A, Chrysant SG, Calhoun D, et al. Renin inhibition with aliskiren provides additive antihypertensive efficacy when used in combination with hydrochlorothiazide. J Hypertens 2007; 25: 217–26
Jordan J, Engeli S, Boye SW, et al. Direct renin inhibition with aliskiren in obese patients with arterial hypertension. Hypertension 2007; 49: 1047–55
Blumenstein M, Romaszko J, Calderon A, et al. Anti-hypertensive efficacy and tolerability of aliskiren/ hydrochlorothiazide (HCT) fixed-dose combination tablets in patients who are non-responsive to HCT 25 mg alone. Curr Med Res Opin 2009; 25: 903–10
Nickenig G, Simanenkov V, Lembo G, et al. Efficacy of aliskiren/hydrochlorothiazide single-pill combinations in aliskiren non-responders. Blood Press 2008; 17Suppl. 2: 31–40
Sica D, Gradman AH, Lederballe O, et al. Aliskiren, a novel renin inhibitor, is well tolerated and has sustained BP-lowering effects alone or in combination with HCTZ during long-term (52 weeks) treatment of hypertension [abstract no. P-797]. Eur Heart J 2006; 27 Suppl.: 121
Pool JL, Schmieder RE, Azizi M, et al. Aliskiren, an orally effective renin inhibitor, provides antihypertensive efficacy alone and in combination with valsartan. Am J Hypertens 2007; 20: 11–20
Krousel-Wood M, Thomas S, Muntner P, et al. Medication adherence: a key factor in achieving blood pressure control and good clinical outcomes in hypertensive patients. Curr Opin Cardiol 2004; 19: 357–62
Burnier M. Medication adherence and persistence as the cornerstone of effective antihypertensive therapy. Am J Hypertens 2006; 19: 1190–6
White WB, Bresalier R, Kaplan AP, et al. Safety and tolerability of the direct renin inhibitor aliskiren: a pooled analysis of clinical experience in more than 12,000 patients with hypertension. J Clin Hypertens 2010; 12: 765–75
Patel BV, Remigio-Baker RA, Mehta D, et al. Effects of initial antihypertensive drug class on patient persistence and compliance in a usual-care setting in the United States. J Clin Hypertens (Greenwich) 2007; 9: 692–700
Weir MR, Flack JM, Applegate WB. Tolerability, safety, and quality of life and hypertensive therapy: the case for low-dose diuretics. Am J Med 1996; 101: 83S–92S
Andersen K, Weinberger MH, Egan B, et al. Comparative efficacy and safety of aliskiren, an oral direct renin inhibitor, and ramipril in hypertension: a 6-month, randomized, double-blind trial. J Hypertens 2008; 26: 589–99
Schmieder RE, Philipp T, Guerediaga J, et al. Long-term antihypertensive efficacy and safety of the oral direct renin inhibitor aliskiren: a 12-month randomized, double-blind comparator trial with hydrochlorothiazide. Circulation 2009; 119: 417–25
Taylor A, Anderson DR, Arora V, et al. Renin system suppression with the oral direct renin inhibitor aliskiren administered alone or in combination: a pooled analysis of 1093 patients with hypertension [abstract no. P-1014-1170]. J Am Coll Cardiol 2007; 49: 370A
Bangalore S, Kamalakkannan G, Parkar S, et al. Fixed-dose combinations improve medication compliance: a meta-analysis. Am J Med 2007; 120: 713–9
Acknowledgements
All authors participated in the development and writing of the paper, and approved the final manuscript for publication. The authors would like to thank Shannon Ritter (Novartis Pharmaceuticals Corporation, East Hanover, NJ, USA) for confirming the data presented in this manuscript. The authors take full responsibility for the content of the paper and thank Dr Jenny Handford (Oxford PharmaGenesis™ Ltd) for medical writing support, editorial assistance, and collation and incorporation of comments from all authors. Novartis Pharmaceuticals Corporation, East Hanover, NJ, USA, funded this work.
This study was funded by Novartis Pharmaceuticals Corporation, East Hanover, NJ, USA. DS has received research grants from CVRx, GlaxoSmithKline, Novartis and Takeda; served on speakers’ bureaus for Novartis; and served as a consultant/on advisory boards for Novartis, Merck, Daiichi Sankyo, Boehringer Ingelheim and CVRx. AHG has received research grants from Novartis; served on speakers’ bureaus for Novartis, Merck, Daiichi Sankyo, AstraZeneca, Pfizer, Boehringer Ingelheim and Forest Laboratories; and served as a consultant/on advisory boards for Novartis, Daiichi-Sankyo, Forest Laboratories, Merck and AstraZeneca. OL has received lecture honoraria from Novartis, Merck and Boehringer Ingelheim. REK has received lecture honoraria from Novartis, Daiichi-Sankyo, Bristol-Myers Squibb, Boehringer Ingelheim, Menarini, Servier, Merck Sharp & Dohme and Berlin Chemie, and has served on advisory boards for Daiichi Sankyo and Boehringer Ingelheim. JZ and DLK are employees of Novartis Pharmaceuticals Corporation, and are thus eligible for Novartis stock and stock options.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Sica, D., Gradman, A.H., Lederballe, O. et al. Long-Term Safety and Tolerability of the Oral Direct Renin Inhibitor Aliskiren with Optional Add-On Hydrochlorothiazide in Patients with Hypertension. Clin. Drug Investig. 31, 825–837 (2011). https://doi.org/10.1007/BF03256921
Published:
Issue Date:
DOI: https://doi.org/10.1007/BF03256921