
Abstract
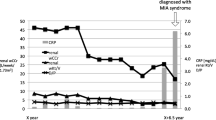
We report, herein, cases of two renal transplantation patients who underwent coronary artery bypass grafting and discuss the perioperative management of this clinical situation. The first case was a 43-year-old male who underwent coronary artery bypass grafting 50 days after renal transplantation, and the second was a chronic case of a 49-year-old male who underwent coronary artery bypass grafting 17 years after renal transplantation. Prior to the operation, the first patient was continuously administered 2mg/kg/day of cyclosporin A with the dosage regulated according to the plasma level. The second patient was administered 50mg/day of cyclophosphamide intravenously instead of an oral dosage of 50mg/day of azathioprine just prior to the operation. In both patients, perfusion pressure during cardiopulmonary bypass was maintained at approximately 80 mmHg in order to obtain optimal urine output. The CD4/CD8 ratio was monitored for indication of graft rejection, but no remarkable changes were observed perioperatively in either patient. Both patients followed a good clinical course and their postoperative renal function was well maintained. The urine output during cardiopulmonary bypass was 300ml and 650ml, respectively. The patients were discharged 15 and 27 days after their operation, respectively. In conclusion, coronary artery bypass grafting can be safely performed in patients who have undergone renal transplantation, if there is appropriate perioperative usage of immunosuppressive agents and maintenance of perfusion pressure during cardiopulmonary bypass.
Similar content being viewed by others

References
Nakhjavan FK, Kahn D, Rosenbaum J, Ablaza S, Goldberg H: Aortocoronary vein graft surgery in a cadaver kidney transplant recipient. Arch Intern Med 1975; 135: 1511–3.
Ando M, Koyanagi H, Endo M, Nishida H, Hachida M, Teraoka S: A report of two cases of coronary bypass surgery after renal transplantation (in Japanese with English abstract). J Jpn Assn Thorac Surg 1993; 41: 2126–30.
Yamamura M, Miyamoto T, Murata H, Kitai K, Ueda T, Wada T. A case of myocardial revascularization in a patient after renal transplantation (in Japanese with English abstract). J Jpn Assn Thorac Surg 1993; 41: 503–8.
Matsumura G, Talanashi Y, Hiramatsu T, Hoshino S, Imai Y, Nakazawa M. A successful mitral valve replacement for a 13-year-old girl with mitral stenosis and pulmonary hypertension after renal transplantation (in Japanese with English abstract). J Jpn Assn Thorac Surg 1997; 45: 985–9.
Eide TR, Belenker S: Effect of cardiopulmonary bypass on plasma cyclosporin A levels in a renal transplant patient. Anesth Analg 1992; 74: 288–90.
Matsumiya G, Nakano S, Shirakura R, Nakata S, Fukushima N, Matsuda H. Aortic valve replacement in a kidney transplant recipient (in Japanese with English abstract). J Jpn Assn Thorac Surg 1994; 42: 956–60.
Cosimi AB, Colvin RB, Burton RC, Rubin RH, Goldstein G, Kung PC, et al. Use of monoclonal antibodies to T-cell subsets for immunologic monitoring and treatment in recipients of renal allografts. N Engl J Med 1981; 305: 308–14.
Bolman RM 3d, Anderson RW, Molina JE, Schwartz JS, Levine B, Simmons RL, et al. Cardiac operations in patients with functioning renal allografts. J Thorac Cardiovasc Surg 1984; 88: 537–43.
Dresler C, Uthoff K, Wahlers T, Kliem V, Schafers J, Oldhafer K, et al. Open heart operations after renal transplantation. Ann Thorac Surg 1997; 63: 143–6.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Noda, H., Fujimura, Y., Gohra, H. et al. Coronary bypass surgery after renal transplantation. Jpn J Thorac Caridovasc Surg 47, 135–140 (1999). https://doi.org/10.1007/BF03217958
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03217958