
Zusammenfassung
Die chronische Canaüculitis kann entweder sekundär nach einer Dacryocystitis auftreten oder aber als primäre Entzündung des oberen oder unteren Canaliculus dem betroffenen Patienten Beschwerden bereiten.
Unsere retrospektive Studie umfaßt 32 Patienten, die an einer isolierten Entzündung des oberen (93,7%) oder unteren (6,3%) Canaliculus litten. Die Zuweisung war in 62,5% der Fälle hauptsächlich zur Abklärung einer einseitigen chronischen Konjunktivitis erfolgt.
Die Pilzkulturen waren in einem Drittel der Fälle positiv, ein weiteres Drittel der abgenommenen Proben zeigte bereits in der Giemsa-Färbung Aktinomyzeten. Der Rest der gewonnenen Isolate zeigte positives Bakterienwachstum (aerob und anaerob).
Das typische klinische Bild, die adäquate Diagnostik, sowie die notwendigen therapeutischen Maßnahmen werden präsentiert und diskutiert.
Summary
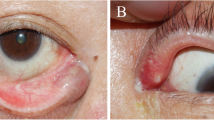
The chronic lacrimal canaliculitis represents an inflammation of the superior or inferior lacrimal canaliculus. The typical clinical findings are a unilateral conjunctivitis, an inflamed eyelid swollen in the region of the lacrimal canaliculus and mucopurolent discharge, as well as dacryoliths, which can be pressed out of the canaliculus.
Our retrospective study enclosed 32 patients, presented with an inflammation of the superior (93.7%) or of the inferior (6.3%) lacrimal canaliculus. The patients were referred to the outpatient clinic of the second department of Ophthalmology of the University of Vienna in 62.5% under the diagnosis of a unilateral chronic conjunctivitis.
Fungi could be isolated in one third of the cases, in another third of the specimens Actinomyces were detected in a Giemsa stain. Anaerob and aerob bacteria were found to be the causative agents in the remaining specimens.
The typical clinical findings, the adequate diagnosis as well as the proper treatment are presented and discussed.
Similar content being viewed by others


Literatur
Barry Al, Garcia F, Trupp LD (1984) An improved single disc method for testing the antibiotic susceptibility of rapidly growing pathogens. Am J Clin Pathol 53: 149–152
Busse H, Müller KM (1977) Zur Entstehung der idiopathischen Dacryostenose. Klin Monatsbl Augenheilkd 170: 627–632
De Concini M, Boi S, Detassis C (1985) Diagnosis and therapy of Actinomycotic lacrimal canaliculitis. Minerva Ophthalmol 27/ 3: 81–83
Huber-Spitzy V, Steinkogler FJ, Huber E, Arocker-Mettinger E, Steurer L, Schiffbänker M (1992) Acquired dacryocystits: Microbiology and conservative treatment. Acta Ophthalmol (in press)
Kanski JJ, Spitznas M (1987) Lehrbuch der klinischen Ophthalmologie. Georg Thieme, Stuttgart New York, S 51–52
Nunery WR, Wilsen II FM (1984) Suppurative canaliculitis. In: Bosnak SL, Smith BC (eds) The lacrimal system. Adv Ophthalmic plast reconstr Surg, vol 3. Pergamo Press, New York, 157–164
Riley SF, Mclachlan DL (1991) Diagnosis and treatment of canaliculitis. Nunery WR.:Ophthalmic plastic and reconstructiv surgery. Ophthalmol clin North Am 4/1: 211–215
Ritleng P, Loubiere R, Marcelet B (1989) Suppurative canaliculitis with concretions. 94 e Congr Soc Fr Ophthalmol Paris, 8–11 mai 198 Ophthalmologie 3/1: 1–3
Struck HG (1981) Zur Problematik der Pilzinfektion der ableitenden Tränenwege. Folia Ophthal, Leipzig 7: 212–216
Struck HG, Höhne C, Tost M (1992) Zur Diagnostik und Therapie der chronischen Canaliculitis. Ophthalmologe 89: 233–236
Wilkins TD, Thiel T (1973) Modified broth-disc method for testing the susceptibility of anaerobic bacteria. Antimicrob Agents Chemother 3: 350–353
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Steurer-Georgiew, L., Huber-Spitzy, V., Huber, E. et al. Diagnose und Therapie der Canaliculitis des Erwachsenen. Spektrum Augeheilkd 7, 25–26 (1993). https://doi.org/10.1007/BF03163890
Issue Date:
DOI: https://doi.org/10.1007/BF03163890