
Summary
We studied the effects of a new approach to breast-feeding infants with phenylketonuria (pku). We compared a group of pku infants being breast-fed according to our new protocol to a group of pku infants receiving formula only. The breast-fed group consisted of nine infants born between 1994 and 1999, being breast-fed at the moment of diagnosis. The formula fed group consisted of nine pku infants, born between 1988 and 1997. In the breast-fed group feedings alternated between breast feeding and phenylalanine-free bottle feeding. The number of breast feedings per day was adapted to the plasma phenylalanine concentrations. At each feeding, whether bottle or breast, the child was allowed to drink until satiety was reached. Data about dietary control and growth during the first six months showed no statistically significant differences, suggesting that this feeding protocol is safe in the strict treatment of otherwise healthy PKU infants.
Samenvatting
Doel van de studie was het evalueren van de effecten van het geven van borstvoeding aan zuigelingen met pku op een andere manier dan internationaal wordt aanbevolen. Wij vergeleken twee groepen zuigelingen met fenylketonurie (pku). Eén groep (n = 9) kreeg borstvoeding volgens een gewijzigd borstvoedingsprotocol, de andere groep (n = 9) kreeg volledig flesvoeding. De voeding in de borstvoedingsgroep bestond uit het in een vast patroon afwisselend geven van een volledige borstvoeding en een volledige fenyl-alaninevrije flesvoeding. Het aantal borstvoedingen werd aangepast aan de fenylalanineconcentraties in het bloed. Bij elke voeding (borstvoeding of flesvoeding) dronk het kind tot het verzadigd was. In de eerste zes maanden na het stellen van de diagnose lieten de resultaten weinig verschillen zien met betrekking tot metabole controle en groei. Het geven van borstvoeding volgens ons protocol lijkt veilig voor gezonde zuigelingen met pku.
Similar content being viewed by others

Notes
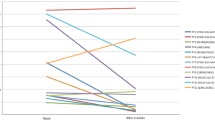
mediaan, spreidingen min/max staan tussen haakjes.
fenylalanine = plasmafenylalanineconcentratie.
Literatuur
Verkerk PH. Twintig jaar landelijke screening op fenylketonurie in Nederland. Ned Tijdschr Geneeskd 1995;139:2302-5.
Schmidt H, Burgard P, Pietz J, et al. Intelligence and professional career in young adults treated early for phenylketonuria. Eur J Pediatr 1996;155:97-100.
Inspectie voor de Gezondheidszorg. Studiegroep Voeding 0-4-jarigen. Voeding van zuigelingen en peuters, uitgangspunten voor de voedingsadvisering voor kinderen van 0-4 jaar. Den Haag: Voedingscentrum, 1999.
Donkers ECMM, Douwes AC, Hammink J. Voedingsadvisering bij jonge kinderen. In: Fernandes J (red.). Ontwikkelingen in de kindervoeding. Assen: Van Gorcum, 1999;5-9.
Vallenas C. Evidence for the ten steps to successful breastfeeding. Geneva: WHO/CHD, 1998.
McCabe ERB, McCabe L. Issues in the dietary management of phenylketonuria: Breast-feeding and trace-metal nutriture. Ann NY Acad Sci 1986;477:215-22.
Acosta PB, Yannicelli S. The Ross metabolic formula system, nutrition support protocols. In: Protocol 1 Phenylketonuria (PKU) (3rd ed.). Columbus, Ohio: Ross Laboratories, 1997; 1-49.
Francis D. Diets for sick children. In: Phenylketonuria (4th ed.). London: Blackwell, 1987;224-262.
Motzfieldt K, Lilje R, Nylander G. Breastfeeding in phenylketonuria. Acta Paediatr 1999;Suppl 432:25-7.
Shaw V, Lawson M. Clinical paediatric dietetics. In: Barnes J. PKU. London: Blackwell, 1995;178-185.
Greve LC, Wheeler MD. Breast-feeding in the management of the newborn with phenylketonuria: a practical approach to dietary therapy. J Am Diet Assoc 1994;94:305-9.
TNO/LUMC. Groeionderzoek 1997. Groeidiagrammen 1997. Houten: Bohn Stafleu Van Loghum, 1998.
Verkerk PH, Spronsen FJ van, Smit GPA, Sengers RCA. Impaired prenatal and postnatal growth in Dutch patients with phenylketonuria. Arch Dis Child 1994;71:114-8.
Willatts P, Forsyth JS. Effect of long-chain polyunsaturated fatty acids in infant formula on problem solving at 10 months of age. Lancet 1998;352:688-91.
Giovanni M, Biasucci G, Agostoni C, et al. Lipid status and fatty acid metabolism in phenylketonuria. J Inherit Metab Dis 1995;18:265-72.
Macdonald A. Factors affecting the variation in plasma phenylalanine in patients with phenylketonuria on diet. Arch Dis Child 1996;74:412-7.
Macdonald A, Rylance G. Does a single plasma phenylalanine predict quality of control in phenylketonuria? Arch Dis Child 1998;78:122-6.
Spronsen FJ van, Rijn M van, Dijk T van, et al. Plasma phenylalanine and tyrosine responses to different nutritional conditions (fasting/postprandial) in patients with phenylketonuria: effect of sample timing. Pediatrics 1993;92:570-3.
Spronsen FJ van, Rijn M van, Dijk T van. Large daily fluctuations in plasma tyrosine in treated patients with phenylketonuria. Am J Clin Nutr 1996;64:916-21.
Gerdes AM, Nielsen JB. Plasma amino acids in phenylketonuric children treated either with phenylalanine-free amino acids or a protein hydrolysate. Acta Paediatr Scand 1990;79:69-72.
Author information
Authors and Affiliations
Additional information
M. van Rijn, afdeling Diëtetiek.
J. Bekhof, afdeling Metabole Ziekten, Kindergeneeskunde Beatrix Kinderkliniek.
T. Dijkstra, afdeling Diëtetiek.
G.P.A. Smit, afdeling Metabole Ziekten, Kindergeneeskunde Beatrix Kinderkliniek.
P. Modderman, Laboratorium Metabole Ziekten.
F.J. van Spronsen, afdeling Metabole Ziekten, Kindergeneeskunde Beatrix Kinderkliniek. Academisch Ziekenhuis Groningen.Correspondentieadres: M. van Rijn, diëtist, afdeling Diëtetiek, Academisch Ziekenhuis Groningen, Postbus 30 001, 9700 RB Groningen.
Rights and permissions
About this article
Cite this article
van Rijn, M., Bekhof, J., Dijkstra, T. et al. Borstvoeding: ook voor het kind met fenylketonurie. KIND 70, 68–71 (2002). https://doi.org/10.1007/BF03061375
Issue Date:
DOI: https://doi.org/10.1007/BF03061375