
Abstract
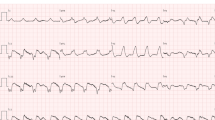
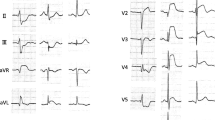
In acute myocardial infarction, early identification of patients at a high mortality risk is important for planning further therapeutic strategies. Previous studies have demonstrated that the extent of carly resolution of ST-segment elevation may represent a simple, quick and noninvasive assessment to identify high risk groups of patients.
In a subgroup of the COBALT Study population (Continuous Infusion vs Double Bolus Administration of Alteplase), ST-segment elevation was measured before and 90 to 120 minutes after treatment with alteplase. The subgroup of n=1,760 patients was not different from the total COBALT population of n=7169 patients regarding most clinical parameters except Killip Class before treatment. However, the overall 30-day mortality differed significantly between the main study and the substudy (7.76% vs 3.52%; p < 0.001).
Three groups of ST-segment resolution were defined: 1. complete resolution (resolution ≥ 70%; 762 patients), 2. partial resolution (< 70% and > 30%; 491 patients), 3. no resolution (< 30%; 507 patients). Mortality rate at 30 days for complete, partial and no resolution of ST-segment elevation was 1.31%, 4.28% and 6.11%, respectively (p < 0.001). While this significant correlation between the extent of ST-segment resolution and mortality could be observed for inferior acute myocardial infarction, it could not be found in patients with anterior acute myocardial infarction. This in part may be due to a selection bias that leads to an extremely divergent mortality rate of anterior acute myocardial infarction in the main study and the substudy (10.1% vs 3.94%; p<0.0001).
Despite this limitation, resolution of ST-segment elevation in acute myocardial infarction after thrombolytic therapy allows to identify patients at a high mortality risk and may help to select patients for early invasive procedures such as PTCA. Patients with complete ST-segment resolution showed a particularly low mortality rate, irrespective of the alteplase regimen used (front-loaded alteplase vs double bolus alteplase).
Zusammenfassung
Die Standardtherapie des akuten Myokardinfarkts ist die Gabe von Thrombolytika oder die akute perkutane transluminale Koronarangioplastie (PTCA). Beide Verfahren haben die schnelle Wiedereröffnung des infarktverursachenden Koronargefäßes zum Ziel. Nur die frühe Wiederherstellung eines nicht kompromittierten Blutflusses im Koronargefäß führt zu einer Verkleinerung der Infarktgröße und einer Verbesserung der Prognose. Im Falle der thrombolytischen Behandlung ist eine rasche nichtinvasive Identifizierung einer erfolgreichen Wiedereröffnung des Koronargefäßes wünschenswert, um im Falle einer fehlenden Reperfusion frühzeitig die Akutkoronarangiographie und PTCA zu planen. Durch mehrere Studien ist die Rückbildung der ST-Segment-Hebung nach Thrombolyse als prädiktiver Mortalitätsparameter herausgearbeitet worden. Die vorliegende Arbeit diente dazu, anhand einer Subgruppe der COBALT-Studie (Continuous Infusion vs. Double Bolus Administration of Alteplase) den Prädiktor ST-Strecken-Rückbildung im EKG 90 bis 120 Minuten nach Therapie mit Alteplase im Vergleich zum Ausgangs-EKG zu untersuchen. Hierzu wurde die ST-Strecken-Hebung vor und 90 bis 120 Minuten nach Behandlung mit Alteplase verglichen. Die Subgruppe von n=1 760 Patienten unterschied sich nach klinischen Kriterien nicht von der COBALT-Gesamtpopulation von n=7 169 Patienten, mit der Ausnahme der Killip-Klasse von Behandlung (Tabelle 1). Trotz der Vergleichbarkeit klinischer Charakteristika ergab sich eine signifikante Differenz in der 30-Tage-Sterblichkeit zwischen der Gesamtstudie und der EKG-Substudie (7,76% vs. 3,52%; p < 0,001).
Es wurden drei Gruppen der Rückbildung der ST-Strecken-Hebung definiert: 1. komplette Rückbildung (Rückbildung > 70%; n=762 Patienten), 2. partielle Rückbildung (<70% and > 30%; n=491 Patienten), 3. keine Rückbildung (<30%; n=507 Patienten; Tabelle 2). Die 30-Tage-Sterblichkeitsrate betrug in der Gruppe der kompletten, der partiellen und der fehlenden ST-Rückbildung 1,31%, 4,28% und 6,11% (p < 0,001; Abbildung 1). Während diese signifikante Assoziation zwischen dem Ausmaß der ST-Strecken-Rückbildung auch in der Untergruppe von Patienten mit inferiorem Myokardinfarkt zu beobachten war, konnte bei Patienten mit anteriorem Myokardinfarkt kein signifikanter Unterschied in der Mortalität zwischen partieller und fehlender ST-Strecken-Rückbildung gefunden werden (Abbildung 2). Dieses kann zumindest teilweise auf eine auffallend divergierende Mortalität des akuten Vorderwandinfarkts in der Hauptstudie und der Substudie zurückgeführt werden (10,1% vs. 3,94%; p < 0,0001). Es wird vermutet, daß die besonders niedrige Mortalität in der Substudie die Ausbildung von signifikanten Unterschieden der Untergruppen unmöglich macht.
Trotz dieser Limitation der vorliegenden Studie bestätigte sich das Ausmaß der ST-Strecken-Rückbildung als Prädiktor der 30-Tage-Mortalität bei Thrombolysetherapie des akuten Myokardinfarkts. Somit kann in Übereinstimmung mit früheren Studien (Tabelle 4, Abbildungen 4 und 5) das Ausmaß der ST-Strecken-Rückbildung als nichtinvasiver Parameter genutzt werden, mit dem eine Auswahl der Patienten für eine Akut-PTCA oder erneute Lyse getroffen werden kann. Patienten mit kompletter Rückbildung der ST-Strecken-Hebung nach thrombolytischer Therapie zeigen eine besonders niedrige Mortalitätsrate, unabhängig vom verwendeten Alteplase-Regime (“front-loaded” Alteplase-Infusion oder Doppelbolus Alteplase; Abbildung 3).
Similar content being viewed by others

References
Barbash GI, Roth A, Hod H, et al. Rapid resolution of ST elevation and prediction of clinical outcome in patients undergoing thrombolysis with alteplase (recombinant tissue-type plasminogen activator): results of the Israeli Study of Early Intervention in Myocardial Infarction. Br Heart J 1990;64:241–7.
Claeys MJ, Bosmans J, Veentrstra L, et al. Determinants and prognostic implications of persistent ST-segment elevation after primary angioplasty for acute myocardial infarction: importance of microvascular reperfusion injury on clinical outcome. Circulation 1999;99:1972–7.
Ellis SG, Ribeiro da Silva E, Heyndrickx G, et al. Randomized comparison of rescue angioplasty with conservative management of patients with early failure of thrombolysis for acute myocardial infarction. Circulation 1994;90:2280–4.
Fibrinolytic Therapy Trialists (FTT) collaborative group. Indications for fibrinolytic therapy in suspected acute myocardial infarction: collaborative overview of early mortality and major morbidity results from all randomised trials of more than 1000 patients. Lancet 1994;343:311–22.
Hackworthyy RA, Vogal MB, Harris PJ. Relationship between changes in ST segment elevation and patency of the infarct-related coronary artery in acute myocardial infarction. Am Heart J 1986;112:279–84.
International Joint Efficacy Comparison of Thrombolytics. Randomized, double-blind comparison of reteplase double-bolus administration with streptokinase in acute myocardial infarction (INJECT): trial to investigate equivalence. Lancet 1995;346:329–36.
Iparraguirre HP, Conti C, Grancelli H, et al. Prognostic value of clinical markers of reperfusion in patients with acute myocardial infarction treated by thrombolytic therapy. Am Heart J 1997; 134:631–8.
Klootwijk P, Langer A, Meij S, et al. Non-invasive prediction of reperfusion and coronary artery patency by continuous ST segment monitoring in the GUSTO-I trial. Eur Heart J 1996; 17:689–98.
Langer A, Krucoff MW, Klootwijk P, et al. Prognostic significance of ST segment shift early after resolution of ST elevation in patients with myocardial infaction treated with thrombolytic therapy: The GUSTO-I ST segment monitoring substudy. J Am Coll Cardiol 1998;31:783–9.
Mauri F, Maggioni AP, Franzosi MG, et al. A simple electrocardiographic predictor of the outcome of patients with acute myocardial infarction treated with a thrombolytic agent. A Gruppo Italiano per lo Studio della Sopravvivenza nellInfarto Miocardico (GISSI-2)-derived analysis. J Am Coll Cardiol 1994;24:600–7.
Pasceri V, Andreotti F, Maseri A. Clinical markers of thrombolytic success. Eur Heart J 1996;17:Suppl E:35–41.
Purcell IF, Newall N, Farrer M. Change in ST segment elevation 60 minutes after thrombolytic initiation predicts clinical outcome as accurately as later electrocardiographic changes. Heart 1997; 78:465–71.
Saran RK, Been M, Furniss SS, et al. Reduction in ST segment elevation after thrombolysis predicts either coronary reperfusion or preservation of left ventricular function. Br Heart J 1990; 64:113–7.
Schröder R, Dissmann R, Brüggemann T, et al. Extent of early ST segment elevation resolution: A simple but strong predictor of outcome in patients with acute myocardial infarction. J Am Coll Cardiol 1994;24:384–91.
Schröder R, Wegscheider K, Schröder K, et al. Exteut of early ST segment elevation resolution: A strong predictor of outcome in patients with acute myocardial infarction and a sensitive measure to compare thrombolytic regimes. A substudy of the International Joint Efficacy Comparison of Thrombolytics (INJECT) Trial. J Am Coll Cardiol 1995;26:1657–64.
Schröder R, Wegscheider K, Neuhaus KL, et al. Significance of initial ST segment changes for thrombolytic treatment in first myocardial infarction. Heart 1997;77:506–11.
Schröder R, Zeymer U, Wegscheider K, et al. Predictive value of ST segment elevation resolution 90 and 180 minutes after start of streptokinase in acute myocardial infarction. A substudy of the Hirudin for Improvement of Thrombolysis (HIT)-4 study. Eur Heart J (in press).
Stewart JT, French JK, Theroux P, et al. Early noninvasive identification of failed reperfusion after intravenous thrombolytic therapy in acute myocardial infarction. J Am Coll Cardiol 1998;31:1499–505.
Tanasijevic MJ, Cannon CP, Wybenga DR, et al. Myoglobin, creatinine kinase MB, and cardiac troponin-I to assess reperfusion after thrombolysis for acute myocardial infarction: Results from TIMI 10A. Am Heart J 1997;134:622–30.
The Continuous Infusion Versus Double-Bolus Administration of Alteplase (COBALT) Investigators. A comparision of infusion of alteplase with double-bolus administration for acute myocardial infarction. N Engl J Med 1997;337:1124–30.
The GUSTO Angiographic Investigators. The effect of tissue plasminogen activator, streptokinase, or both on coronary artery patency, left ventricular function, and survival after acute myocardial infarction. N Engl J Med 1993;329:1615–22.
The ISAM Study Group. A prospective trial of intravenous streptokinase in acute myocardial infarction (ISAM). Mortality, morbidity, and infarct size at 21 days. N Engl J Med 1986;314:1465–71.
van’t Hof AWJ, Liem A, de Boer MJ, et al. Clinical value of 12-lead electrocardiogram after successful reperfusion therapy for acute myocardial infarction. Lancet 1997;350:615–9.
Wegscheider K, Neuhaus KL, Dissmann R, et al. Prognostische Bedeutung der ST-Streckenveränderung beim akuten Myokardinfarkt. Herz 1999;24:378–88.
Zeymer U, Schröder R, Neuhaus KL. Patency, Perfusion und Prognose beim akuten Herzinfarkt. Herz 1999;24:421–9.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Carlsson, J., Kamp, U., Härtel, D. et al. Resolution of ST-segment elevation in acute myocardial infarction — Early prognostic significance after thrombolytic therapy. Herz 24, 440–447 (1999). https://doi.org/10.1007/BF03044430
Issue Date:
DOI: https://doi.org/10.1007/BF03044430