
Abstract
Purpose: To assess how completely anesthesiologists check their machinery and equipment before use, and to determine what influence seniority, age and type of practice may have on checking practices.
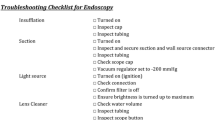
Methods: One hundred and twenty anesthesiologists were videotaped during a simulated anesthesia session. Each participant was scored by an assessor according to the number of items checked prior to the induction of anesthesia. A checklist of 20 items derived from well-publicized, international standards was used.
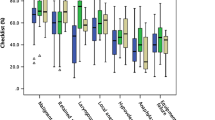
Results: Participants were grouped according to their type of practice. Overall, mean scores were low. The ideal score was 20. There were no differences among university anesthesiologists (mean score 10.1, standard deviation 4.3), community anesthesiologists (7.5±4.3) and anesthesia residents (9.0±3.8). Each of these groups scored, on average, better than medical students (3.6±3.7) (P<0.05). Neither age (r=0.15,P>0.1) nor number of years in practice (r=−0.18,P>0.1) correlated with score.
Conclusions: Our study suggests that the equipment-checking practices of anesthesiologists require considerable improvement when compared with national and international standards. Possible reasons for this are discussed and some remedial suggestions are made.
Résumé
Objectif: Évaluer le degré de vérification des appareils faite par les anesthésiologistes avant de les utiliser et déterminer l’influence de l’ancienneté, de l’âge et du type de pratique sur les habitudes de vérification.
Méthode: Cent vingt anesthésiologistes ont été filmés sur vidéocassette pendant une session d’anesthésie simulée. Chaque participant a été coté par un évaluateur selon le nombre d’éléments vérifiés avant l’induction de l’anesthésie. On a utilisé une liste de 20 éléments dérivée de normes internationales bien connues.
Résultats: Les participants ont été regroupés selon leur type de pratique. Globalement, les scores moyens ont été faibles. Le meilleur score a été de 20. Il n’y avait pas de différence entre les anesthésiologistes spécialistes (moyenne de 10,1 et écart type de 4,3). les anesthésiologistes omnipraticiens (7,5±4,3) et les résidents en anesthésie (9,0±3,8). Chacun de ces groupes a affiché des scores moyens meilleurs que ceux des étudiants de médecine (3,6±3,7) (P<0,05). Il n’y avait pas de corrélation entre l’âge (r=0,15,P>0,1) ou le nombre d’années d’exercice (r=−0,18,P>0,1) et le score obtenu.
Conclusion: Notre étude permet de présumer que les habitudes de vérification de l’équipement des anesthésiologistes, comparées aux normes nationales et internationales, doivent être de beaucoup améliorées. Les causes possibles de cette situation sont examinées et certaines solutions sont proposées.
Article PDF
Similar content being viewed by others

References
Cooper JB, Newbower RS, Kitz RJ. An analysis of major errors and equipment failures in anesthesia management: considerations for prevention and detection. Anesthesiology 1984; 60: 34–42.
Craig J, Wilson ME. A survey of anaesthetic misadventures. Anaesthesia 1981; 36: 933–6.
Heath ML. Accidents associated with equipment. Anaesthesia 1984; 39: 57–60.
Webb RK, Russell WJ, Klepper I, Runciman WB. Equipment failure: an analysis of 2000 incident reports. Anaesth Intensive Care 1993; 21: 673–7.
United States Food and Drug Administration. Anesthesia apparatus checkout recommendations, 1993. Rockville, MD: Federal Register, February 1987.
Association of Anaesthetists of Great Britain and Ireland. Checklist for anaesthetic apparatus. A recommended procedure based on the use of an oxygen analyser. London: Association of Anaesthetists of Great Britain and Ireland, 1990.
Australian and New Zealand College of Anaesthetists. Protocol for checkiong the anaesthetic machine. Melbourne: Australian and New Zealand College of Anaesthetists, 1997.
Canadian Anesthesiologists’ Society. CAS Guidelines to the practice of anesthesia. Toronto: Canadian Anesthesiologists’ Society, 1998.
Mayor AH, Eaton, JM. Anaesthetic machine checking practices. A survey. Anaesthesia 1992; 47: 866–8.
Clayton DG, Barker L, Runciman WB. Evaluation of safety procedures in anaesthesia and intensive care. Anaesth Intensive Care 1993; 21: 670–2.
Olympio MA, Goldstein MM, Mathes DD. Instructional review improves performance of anesthesia apparatus checkout procedures. Anesth Analg 1996; 83: 618–22.
Kurrek MM, Devitt JH. The cost for construction and operation of a simulation centre. Can J Anaesth 1997; 44: 1191–5.
Devitt JH, Kurrek M, Cohen M. Participants’ evaluation of a simulator based evaluation. Anesthesiology 1999; 91: A1131.
Groves J, Edwards N, Carr B. The use of a visual aid to check anaesthetic machines. Is performance improved? Anaesthesia 1994; 49: 122–5.
Cundy J, Baldock GJ. Safety check procedures to eliminate faults in anaesthetic machines. Anaesthesia 1982; 37: 161–9.
March MG, Crowley JJ. An evaluation of anesthesiologists’ present checkout methods and the validity of the FDA checklist. Anesthesiology 1991; 75: 724–9.
Webb RK, van der Walt JH, Runciman WB, et al. Which monitor? An analysis of 2000 incident reports. Anaesth Intensive Care 1993; 21: 529–42.
Adams AP, Morgan M. Checking anaesthetic machines — checklists or visual aids? (Editorial) Anaesthesia 1993; 48: 183–6.
Manley R, Cuddeford JD. An assessment of the effectiveness of the revised FDA checklist. AANA Journal 1996; 64: 277–82.
Jackson IJB, Wilson RJT. Association of Anaesthetist’s checklist for anaesthetic machines. Problem with detection of significant leaks. Anaesthesia 1993; 48: 152–3.
Berge JA, Gramstad L, Grimnes S. An evaluation of a time-saving anaesthetic machine checkout procedure. Eur J Anaesthesiol 1994; 11: 493–8.
Berge JA, Gramstad L, Jensen Ø. A training simulator for detecting equipment failure in the anaesthetic machine. Eur J Anaesthesiol 1993; 10: 19–24.
Runciman WB, Sellen A, Webb RK et al. Errors, incidents and accidents in anaesthetic practice. Anaesth Intensive Care 1993; 21: 506–19.
Barthram C, McClymont W. The use of a checklist for anaesthetic machines. Anaesthesia 1992; 47: 1066–9.
Author information
Authors and Affiliations
Additional information
Supported with a grant from the Physicians of Ontario through the Physicians Services Incorporated Foundation. Dr Cohen is the recipient of a Senior Scientist Award from the Medical Research Council of Canada.
Rights and permissions
About this article
Cite this article
Armstrong-Brown, A., Devitt, J.H., Kurrek, M. et al. Inadequate preanesthesia equipment checks in a simulator. Can J Anesth 47, 974–979 (2000). https://doi.org/10.1007/BF03024868
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03024868