
Abstract
Purpose: To evaluate the effect of adding clonidine to ropivacaine, for axillary brachial plexus blockade, on the onset and duration of sensory and motor block and duration of analgesia.
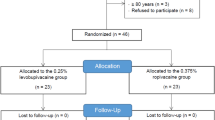
Methods: In a prospective randomised double blind placebo controlled study axillary brachial plexus blockade was performed in 50 patients using 40 ml ropivacaine 0.75%. Group (A) had 150µg donidine and Group (B) 1 ml normal saline added to the local anesthetic. Sensory function was tested using pinprick (sharp sensation, blunt sensation or no sensation) and temperature with an ice cube compared with the opposite arm, (cold/not cold). Motor function was assessed using a modified Bromage scale. Postoperative analgesia was standardised. Onset and duration of sensory and motor blockade, duration of analgesia, postoperative pain score, and analgesic requirement were compared.
Results: The clonidine patients showed an increase in duration of sensory loss from 489 min to 628 min with a mean difference of 138 min (95% confidence interval of 90 to 187 min), motor blockade from 552 min to 721 min with a mean difference of 170 min (95% confidence interval of 117 to 222 min), and analgesia from 587 min to 828 min with mean difference of 241 min (95% confidence interval of 188 to 294 min). There was no difference in onset time. No side effects were noted.
Conclusion: The addition of 150µg of clonidine to ropivacaine, for brachial plexus blockade, prolongs motor and sensory block and analgesia, without an increased incidence of side effects.
Résumé
Objectif: Évaluer l’effet d’un ajout de clonidine à la ropivacaïne, pour le blocage du plexus brachial axillaire, sur le délai d’installation et la durée du bloc sensitif et moteur et sur la durée de l’analgésie.
Méthode: Il s’agit d’une étude prospective, randomisée et à double insu contre placebo. Un blocage du plexus brachial axillaire a été réalisé chez 50 patients en utilisant 40 ml de ropivacaïne à 0,75%. On a ajouté à l’anesthésique local, 150µg de clonidine pour les patients du groupe A et 1 ml de solution salée pour ceux du grupe B. La fonction sensitive a été testée par piqûre d’épingle (sensation vive, légère sensation ou insensibilité) et la température par un cube de glace posé en alternance sur les deux bras (froid, non froid). La fonction motrice a été évaluée avec une étchelle de Bromage modifiée. L’analgésie postopératorie a été normalisée. On a comparé le délai d’installation et la durée du blocage sensitif et moteur, la durée de l’analgésie, le score de douleur postopératoire et les besoins analgésiques.
Réasultats: Chez les patients qui ont reçu de la clonidine, on a noté une perte sensitive de plus longue durée, de 489 min à 628 min avec une différence moyenne de 138 min (intervalle de confinance de 95%, de 90 à 187 min), un blocage moteur plus long de 552 min à 721 min avec une différence moyenne de 170 min (IC de 95%, de 117 à 222 min) et une meilleure analgésie de 587 min à 828 min avec une différence moyenne de 241 min (IC de 95%, de 188 à 294 min). Il n’y a pas eu de différence de délai d’installation. Aucun effet secondaire n’a été enregistré.
Conclusion: L’ajout de 150µg de clonidine à la ropivacaïne, pour un blocage du plexus brachial, prolonge le bloc moteur et sensitif et l’analgésie sans augmenter les effets secondaires.
Article PDF
Similar content being viewed by others


References
Yousef MS, Desgrand DA. Comparison of two methods of axillary brachial plexus anaesthesia. Br J Anaesth 1988; 60: 841–4.
Brockway MS, Wildsmith JAW. Axillary brachial plexus block: method of choice? Br J Anaesth 1990; 64: 224–31.
McClure JH. Ropivacaine. Br J Anaesth 1996; 76: 300–7.
Cederholm I, Anskär S, Bengtsson M. Sensory, motor, and sympathetic block during epidural analgesia with 0.5% and 0.75% ropivacaine with and without epinephrine. Reg Anesth 1994; 19: 18–33.
Hickey R, Blanchard J, Hoffman J, Sjovall J, Ramamurthy S. Plasma concentrations of ropivacaine given with or without epinephrine for brachial plexus block. Can J Anaesth 1990; 37: 878–82.
Maze M, Tranquilli W. Alpha 2 adrenoceptor agonists: defining the role in clinical anesthesia. Anesthesiology 1991; 74: 581–605.
Racle JP, Benkhadra A, Poy JY, Gleizal B. Prolongation of isobaric bupivacaine spinal anesthesia with epinephrine and clonidine for hip surgery in the elderly. Anesth Analg 1987; 66: 442–6.
Bernard J-M, Macaire P. Dose-range effects of clonidine added to lidocaine for brachial plexus block. Anesthesiology 1997; 87: 277–84.
Eledjam JJ, Deschodt J, Viel EJ, et al. Brachial plexus block with bupivacaine: effects of added alpha- adrenergic agonists: comparison between clonidine and epinephrine. Can J Anaesth 1991; 38: 870–5.
Gaumann D, Foster A, Griessen M, Habre W, Poinsot O, Della Santa D. Comparison between clonidine and epinephrine admixture to lidocaine in brachial plexus block. Anesth Analg 1929; 75: 69–74.
Singelyn FJ, Dangoisse M, Bartholomée S, Gouverneur JM. Adding clonidine to mepivacaine prolongs the duration of anesthesia and analgesia after axillary brachial plexus block. Reg Anesth 1992; 17: 148–50.
Singelyn FJ, Gouverneur J-M, Robert A. A minimum dose of clonidine added to mepivacaine prolongs the duration of anesthesia and analgesia after axillary brachial plexus block. Anesth Analg 1996; 83: 1046–50.
Pertovaara A, Kauppila T, Jyväsjärvi E, Kalso F. Involvement of supraspinal and spinal segmental alpha-2- adrenergic mechanisms in the medetomidine-induced antinociception. Neuroscience 1991; 44: 705–14.
Samsó E, Vallés J, Pol O, Gallart L, Puig MM. Comparative assessment of the anesthetic and analgesic effects of intramuscular and epidural clonidine in humans. Can J Anaesth 1996; 43: 1195–202.
De Kock M, Gautier P, Pavlopoulou A, Jonniaux M, Lavand’homme P. Epidural clonidine or bupivacaine as the sole analgesic agent during and after abdominal surgery. Anesthesiology 1999; 90: 1354–62.
Sarantopoulos C, Fassoulaki A. Systemic opioids enhance the spread of sensory analgesia produced by intrathecal lidocaine. Anesth Analg 1994; 79: 94–7.
Liu S, Chiu AA, Carpenter RL, et al. Fentanyl prolongs lidocaine spinal anesthesia without prolonging recovery. Anesth Analg 1995; 80: 730–4.
Sia S, Lepri A. Clonidine administered as an axillary block does not affect postoperative pain when given as the sole analgesic. Anesth Analg 1999; 88: 1109–12.
Gordh T Jr,Feuk U, Norlén K. Effects of epidural clonidine on spinal cord blood flow and regional and central hemodynamics in pigs. Anesth Analg 1986; 65: 1312–8.
Butterworth JF IV, Strichartz GR. The alpha2 adrenergic agonists clonidine and guanfacine produce tonic and phasic block of conduction in rat sciatic nerve fibers. Anesth Analg 1993; 76: 295–301.
Gaumann DM, Brunet PC, Jirounek P. Clonidine enhances the effect of lidocaine on C fiber action potential. Anesth Analg 1992; 74: 719–25.
Cockings E, Moore PL, Lewis RC. Transarterial brachial plexus blockade using high doses of 1.5% mepivacaine. Reg Anesth 1987; 12: 159–64.
Vaghadia H, Chan V, Ganapathy S, Lui A, McKenna J, Zimmer K. A multicentre trial of ropivacaine 7.5 mg·ml−1vs bupivacaine 5 mg·ml−1 for supra clavicular brachial plexus anesthesia. Can J Anesth 1999; 46: 946–51.
Astra Zeneca Phrmaceutical Limited. Ropivacaine. Summary of product characteristics. UK 16/6/99.
Brown DL, Carpenter RL, Thompson GE. Comparison of 0.5% ropivacaine and 0.5% bupivacaine for epidural anesthesia in patients undergoing lower-extremity surgery. Anesthesiology 1990; 72: 633–36.
Gentili M, Bernard J-M, Bonnet F. Adding clonidine to lidocaine for intravenous regional anesthesia prevents tourniquet pain. Anesth Analg 1999; 88: 1327–30.
Author information
Authors and Affiliations
Corresponding author
Additional information
Financial Support: NHS Culyer Research Grant
Rights and permissions
About this article
Cite this article
El Saied, A.H., Steyn, M.P. & Ansermino, J.M. Clonidine prolongs the effect of ropivacaine for axillary brachial plexus blockade. Can J Anesth 47, 962–967 (2000). https://doi.org/10.1007/BF03024866
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03024866