
Abstract
The length and method of measurement of the safety-margin below the rectal cancer, being of the utmost importance for its prognosis, is still under debate. The following study was designed and done for its solution.
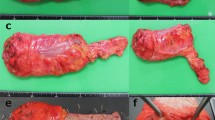
Light microscopic examination was done on 83 resected rectal cancer specimens to assess the extent of intramural invasion towards the anus. By use of a ruler, the distance between the lower tumour margin and the resection line or the dentate line was measured when the specimen was: 1. freshly resected, 2. after fixing in 10% formalin, and 3. after being mounted in sections. The measurements were compared. By the same method, the distance between the lower tumor margin and the intended resectyion line was measured immediately before resection. It was compared with the measurement immediately after the resection.
In 83 rectal cancer specimens, the extent of intramural infiltration toward the anus was: <-0.5 cm in 75 cases (90.4%). ≥1 cm in 2 cases which showed highly malignant carcinomas. These 2 cases, however, should not have been indicated for anus-saving resection. In 46 fresh specimens, the tumor-resection line distances gave an average of 2.7 cm. After fixing in 10% formalin, they became shortened by 0.7 cm. And, mouting in sections further shortened them by another 0.5 cm, giving a total shortening of 1.2 cm. The tumor-resection line distance in 7 of the 11 fresh specimens resected by the Dixon’s operation was shortened, though never more than o.5 cm immediately the operation.
In performin ganus-saving resection for the low rectal cancer, after full isolation the rectum and stretching it slightly, ≥3 cm of the rectum distal to the lower tumor margin should be resected. A safety margin of more than 2.5 cm is necessary in the fresh specimen. If formalin fixed specimen is measured, the safety margin should be ≥2 cm.
Similar content being viewed by others

References
Williams NS, Durdey P, Jchnston D. The outcome following sphinctersaving resection and abdominoperineal resection for low rectal cancer. Br J Surg 1985; 72: 595.
McDermott F, Hughes SE, Pihl E, et al. Long-term results of restorative resection and total excision for carcinoma of the middke third of the rectum. SGO 1982; 154:833.
Nicholls RJ, Ritchie JK, Wadsworth J, et al. Total excision or restorative resection for carcinoma of the middle third of the rectum. Br J Surg 1979; 66:625.
Williams NS, Johnston D. Surgical and recurrence after sphincter saving resection and abdominloperineal resection for carcinoma of the middle third of the rectum. Br J Surg 1984; 71:278.
Elliot MS, Todd JP, Nicholls RJ. Radical restorative surgery for poorly differentiated carcinoma of the mid-rectum. Br J Surg 1982; 69:273.
Williams NS, Dixon MF, Johnston D. Reappraisal of the 5 centimetre rule of distal excision for carcinoma of the rectum: a study of distal intramural spread and of patients’ survival. Br J Surg 1983; 70:150.
Williams NS. The rationale for preservation of the anal sphincter in patients with low rectal cancer. Br J Surg 1984; 71:575.
Black WA, Waugh JM. The intramural extension of carcinoma of the descending colon, sigmoid, and rectosigmoid. SGO 1948; 87:457.
1987; 7(4):167
1983; 21(12):731
1989; 9(11):610
1989; 11(3):213
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Zhang, B., Li, L. Safety margin in anus-saving resection for low rectal cancer. Chin J Cancer Res 7, 209–213 (1995). https://doi.org/10.1007/BF03023476
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03023476