
Abstract
Purpose
Recent warnings regarding the safety of droperidol have limited use of this drug as an antiemetic. Haloperidol, a butyrophenone derivative similar to droperidol, has not been rigorously evaluated as an antiemetic. The aim of this study was to compare the prophylactic antiemetic efficacy of haloperidolvs ondansetron for the prevention of postoperative nausea and vomiting (PONV) after general anesthesia.
Methods
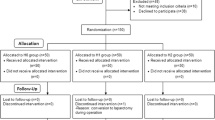
Ninety non-smoking female patients were eligible to participate in this randomized double-blinded study. Approximately 30 min before the end of surgery, patients were randomly assigned to receive either haloperidol 2 mgiv, or ondansetron 4 mgiv, respectively. The incidence of PONV, average pain and sedation scores, recovery times, and changes of the rate-corrected QT (QTc) interval were observed post-operatively.
Results
The proportion of patients who experienced PONV in the first 24 hr was similar in the two groups (28% and 26% for haloperidol and ondansetron groups, respectively). The incidence of PONV was significantly less in both groups than predicted according to the patients’ underlying risks (53% for the haloperidol group,P = 0.016; 51 % for the ondansetron group,P = 0.015). Pain scores, sedation scores, and recovery times were similar in the two groups, and no prolongation of the QTc interval was observed in either group.
Conclusions
Haloperidol 2 mgiv given 30 min before the end of surgery is effective in preventing PONV, with efficacy comparable to ondansetron 4 mgiv for the first 24 hr after general anesthesia.
Résumé
Objectif
De récentes mises en garde quant à l’innocuité du dropéridol ont limité l’utilisation de ce médicament comme antiémétique. L’halopéridol, un dérivé du butyrophénone similaire au dropéridol, n’a pas été évalué rigoureusement en tant qu’antiémétique. L’objectifde cette étude était de comparer l’efficacité antiémétique prophylactique de l’halopéridol vs l’ondansétron dans la prévention des nausées et vomissements postopératoires (PONV) après une anesthésie générale.
Méthode
Quatre-vingt-dix patientes non fumeuses satisfaisaient aux conditions de participation à cette étude randomisée à double insu. Environ 30 min avant la fin de la chirurgie, les patientes ont été randomisées à recevoir respectivement soit 2 mg iv d’halopéridol, soit 4 mg iv d’ondansétron. Après l’opération, l’incidence de PONV, les moyennes des scores de douleur et de sédation, les temps de rétablissement et les changements de l’intervalle QT à taux corrigé (QTc) ont été observés.
Résultats
La proportion de patientes souffrant de PONV dans les premières 24 h était semblable dans les deux groupes (28 % et 26 % pour les groupes halopéridol et ondansétron respectivement). L’incidence de PONV était significativement plus basse que prévue dans les deux groupes en considérant les risques préopératoires sous-jacents des patientes (53 % pour le groupe halopéridol, P = 0,016 ; 51 % pour le groupe ondansétron, P = 0,015). Les scores de douleur et de sédation, ainsi que les temps de rétablissement étaient similaires dans les deux groupes, et aucune prolongation de l’intervalle QTc n’a été observée dans l’un ou l’autre groupe.
Conclusion
L’halopéridol 2 mg iv administré 30 min avant la fin de la chirurgie est efficace dans la prévention de PONV, et présente une efficacité comparable à l’ondansétron 4 mg iv durant les premières 24 h après une anesthésie générale.
Article PDF
Similar content being viewed by others


Avoid common mistakes on your manuscript.
References
Myles PS, Williams DL, Hendrata M, Anderson H, Weeks AM. Patient satisfaction after anaesthesia and surgery: results of a prospective survey of 10,811 patients. Br J Anaesth 2000; 84: 6–10.
Tramer MR. A rational approach to the control of postoperative nausea and vomiting: evidence from systemic reviews. Part II. Recommendations for prevention and treatment, and research agenda. Acta Anaesthesiol Scand 2001; 45: 14–9.
Gan TJ, White PF, Scuderi PE, Watcha MF, Kovac A. FDA “black box” warning regarding use of droperidol for postoperative nausea and vomiting: is it justified? Anesthesiology 2002; 97: 287.
Mullins M, Van Zwieten K, Blunt JR. Unexpected cardiovascular deaths are rare with therapeutic doses of droperidol. Am J Emerg Med 2004; 22: 27–8.
Buttner M, Walder B, von Elm E, Tramer MR. Is low-dose haloperidol a useful antiemetic? A meta-analysis of published and unpublished randomized trials. Anesthesiology 2004; 101: 1454–63.
Vella-Brincat J, Macleod AD. Haloperidol in palliative care. Palliat Med 2004; 18: 195–201.
Apfel CC, Roewer N, Korttila K. How to study postoperative nausea and vomiting. Acta Anaesthesiol Scand 2002; 46: 921–8.
Wang JJ, Ho ST, Lee SC, Liu YC, Ho CMl. The use of dexamethasone for preventing postoperative nausea and vomiting in females undergoing thyroidectomy: a dose-ranging study. Anesth Analg 2000; 91: 1404–7.
Chernik DA, Gillings D, Laine H, et al. Validity and reliability of the Observer’s Assessment of Alertness/ Sedation Scale: study with intravenous midazolam. J Clin Psychopharmacol 1990; 10: 244–51.
Barton MD, Libonati M, Cohen PJ. The use of haloperidol for treatment of postoperative nausea and vomiting — a double-blind placebo-controlled trial. Anesthesiology 1975; 42: 508–12.
Rusch D, Eberhart L, Biedler A, DethlingJ, Apfel CC. Prospective application of a simplified risk score to prevent postoperative nausea and vomiting. Can J Anesth 2005; 52: 478–84.
Lerman J. Study design in clinical research: sample size estimation and power analysis. Can J Anaesth 1996; 43: 184–91.
Tang J, Wang B, White PF, Watcha MF, Qi J, Wender RH. The effect of timing of ondansetron administration on its efficacy, cost-effectiveness, and cost-benefit as a prophylactic antiemetic in the ambulatory setting. Anesth Analg 1998; 86: 274–82.
Parlow JL, Costache J, Avery N, Turner K. Single-dose haloperidol for the prophylaxis of postoperative nausea and vomiting after intrathecal morphine. Anesth Analg 2004; 98: 1072–6.
Aouad MT, Siddik-Sayyid SM, Taha SK, et al. Haloperidol vs. ondansetron for the prevention of postoperative nausea and vomiting following gynaecological surgery. Eur J Anaesthesiol 2007; 24: 171–8.
Henzi I, Sonderegger J, Tramer MR. Efficacy, dose-response, and adverse effects of droperidol for prevention of postoperative nausea and vomiting. Can J Anesth 2000; 47: 537–51.
Gan TJ, Meyer T, Apfel CC, et al.;Department of Anesthesiology, Duke University Medical Center. Consensus guidelines for managing postoperative nausea and vomiting. Anesth Analg 2003; 97: 62–71.
Apfel CC, Kranke P, Katz MH, et al. Volatile anaesthetics may be the main cause of early but not delayed postoperative vomiting: a randomized controlled trial of factorial design. Br J Anaesth 2002; 88: 659–68.
Perrault LP, Denault AY, Carrier M, Cartier R, Belisle S. Torsades de pointes secondary to intravenous haloperidol after coronary bypass grafting surgery. Can J Anesth 2000; 47: 251–4.
Sharma ND, Rosman HS, Padhi ID, Tisdale JE. Torsades de pointes associated with intravenous haloperidol in critically ill patients. Am J Cardiol 1998; 81: 238–40.
Benedict CR, Arbogast R, Martin L, Patton L, Morrill B, Hahne W. Single-blind study of the effects of intravenous dolasetron mesylate versus ondansetron on electrocardiographic parameters in normal volunteers. J Cardiovasc Pharmacol 1996; 28: 53–9.
Kasinath NS, Malak O, Tetzlaff J. Atrial fibrillation after ondansetron for the prevention and treatment of postoperative nausea and vomiting: a case report. Can J Anesth 2003; 50: 229–31.
Baguley WA, Hay WT, Mackie KP, Cheney FW, Cullen BF. Cardiac dysrhythmias associated with the intravenous administration of ondansetron and metoclopramide. Anesth Analg 1997; 84: 1380–1.
Charbit B, Albaladejo P, Funck-Brentano C, Legrand M, Samain E, Marty J. Prolongation of QTc interval after postoperative nausea and vomiting treatment by droperidol or ondansetron. Anesthesiology 2005; 102: 1094–100.
White PF, Watcha MF. Are new drugs cost-effective for patients undergoing ambulatory surgery? Anesthesiology 1993; 78: 2–5.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Lee, Y., Wang, P.K., Lai, H.Y. et al. Haloperidol is as effective as ondansetron for preventing postoperative nausea and vomiting. Can J Anesth 54, 349–354 (2007). https://doi.org/10.1007/BF03022656
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03022656