
Abstract
Purpose
Analgesia and sedation, routinely used as adjunct medications for regional anesthesia, are rarely used in the pregnant patient because of concerns about adverse neonatal effects. In an effort to obtain more information about maternal analgesia and sedation we studied neonatal and maternal effects of iv fentanyl and midazolam prior to spinal anesthesia for elective Cesarean section.
Methods
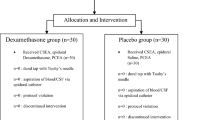
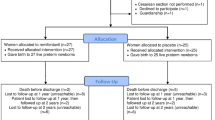
In this double-blinded, randomized, placebo-controlled trial, 60 healthy women received either a combination of 1 µg·kg-1 fentanyl and 0.02 mg·kg-1 midazolam intravenously or an equal volume of iv saline at the time of their skin preparation for a bupivacaine spinal anesthetic. Sample size was based on a non-parametric power analysis (power > 0.80 and alpha = 0.05) for clinically important differences in Apgar scores. Fetal outcome measures included Apgar scores, continuous pulse oximetry for three hours, and neurobehavioural scores. Maternal outcomes included catecholamine levels, and recall of anesthesia and delivery.
Results
There were no between-group differences of neonatal outcome variables (Apgar score, neurobehavioural scores, continuous oxygen saturation). Mothers in both groups showed no difference in their ability to recall the birth of their babies.
Conclusions
Maternal analgesia and sedation with fentanyl (1 µg·kg-1) and midazolam (0.02 mg·kg-1) immediately prior to spinal anesthesia is not associated with adverse neonatal effects.
Résumé
Objectif
Ľanalgésie et la sédation, complément habituel à ľanesthésie régionale, sont rarement utilisées chez la femme enceinte parce qu’on craint les effets néonatals indésirables. Pour en savoir davantage sur ľanalgésie et la sédation de la mère, nous avons étudié les effets sur la mère et ľenfant du fentanyl et du midazolam iv administrés avant la rachianesthésie pour césarienne.
Méthode
Pour ľétude randomisée, à double insu et contrôlée contre placebo, 60 femmes en santé ont reçu une combinaison intraveineuse de 1 µg·kg-1 de fentanyl et 0,02 mg·kg-1 de midazolam ou un volume égal de solution saline iv au moment de préparer à la rachianesthésie avec bupivacaine. La taille de ľéchantillon reposait sur une analyse de puissance non paramétrique (puissance > 0,80 et alpha = 0,05) pour des différences cliniquement importantes ďindices ďApgar. Les mesures de ľévolution du fœtus comprenaient ľindice ďApgar, la sphygmo-oxymétrie continue pendant trois heures et les scores neurocomportementaux. Ľévaluation de la mère incluait les niveaux de catécholamine et la présence de souvenir de ľanesthésie et de ľaccouchement.
Résultats
Il n’y a pas eu de différence intergroupe des variables mesurées chez le nouveau-né (indice ďApgar, comportement neurologique, mesure continue de la saturation en oxygène). Les mères des deux groupes ont montré la même capacité à se rappeler la naissance de leurs enfants.
Conclusion
Ľanalgésie et la sédation maternelles avec du fentanyl (1 µg·kg-1) et du midazolam (0,02 mg·kg-1) administrées immédiatement avant la rachianesthésie ne sont pas associées à des effets néonatals indésirables.
Article PDF
Similar content being viewed by others

Avoid common mistakes on your manuscript.
References
National Institute of Child Health and Human Development (NICHD) Request for Application. Obstetric-Fetal Pharmacology Research Units RFA: HD-03-017. July 29, 2003. National Institutes of Health (http://grants2.nih.gov/grants/guide/rfa-files/FRA-HD-03-017.html).
Camann W, Cohen MB, Ostheimer GW. Is midazolam desirable for sedation in parturients? (Letter). Anesthesiology 1986; 65: 441.
Seidman SF, Marx GF. Midazolam in obstetric anesthesia (Letter). Anesthesiology 1987; 67: 443–4.
Wilson CM, Dundee JW, Moore J, Howard PJ, Collier PS. A comparison of the early pharmacokinetics of midazolam in pregnant and nonpregnant women. Anaesthesia 1987; 42: 1057–62.
DeFrances CJ, Hall MJ. 2002 National Hospital Discharge Survey. Adv Data 2004; 21: 1–29.
Wakefield ML. Systemic analgesia: parenteral and inhalation agents.In: Chestnut D (Ed.). Obstetric Anesthesia: Principles and Practice. Philadelphia: Elsevier Mosby; 2004: 311–23.
Mattingly JE, D’Alessio J, Ramanathan J. Effects of obstetric analgesics and anesthetics on the neonate. A review. Paediatr Drugs 2003; 5: 615–27.
Bricker L, Lavender T. Parenteral opioids for labor pain relief: a systematic review. Am J Obstet Gynecol 2002; 186: S94–109.
Rosaeg OP, Kitts JB, Koren G, Byford LJ. Maternal and fetal effects of intravenous patient-controlled fentanyl analgesia during labour in a thrombocytopenic parturient. Can J Anaesth 1992; 39: 277–81.
Rout CC, Rocke DA. Effects of alfentanil and fentanyl on induction of anaesthesia in patients with severe pregnancy-induced hypertension. Br J Anaesth 1990; 65: 468–74.
Ravlo O, Carl P, Crawford ME, Bach V, Mikkelsen BO, Nielsen HK. A randomized comparison between midazolam and thiopental for elective cesarean section anesthesia: II. Neonates. Anesth Analg 1989; 68: 234–7.
Cheng YJ, Wang YP, Fan SZ, Liu CC. Intravenous infusion of low dose propofol for conscious sedation in cesarean section before spinal anesthesia. Acta Anaesthesiol Sin 1997; 35:79–84; Erratum 1997; 35: 191.
Rayburn W, Rathke A, Leuschen MP, Chleborad J, Weidner W. Fentanyl citrate analgesia during labor. Am J Obstet Gynecol 1989; 161: 202–8.
Atkinson BD, Truitt L J, Rayburn WF, Turnbull GL, Christensen HD, Wlodaver A. Double-blind compari- son of intravenous butorphanol (Stadol) and fentanyl (Sublimaze) for analgesia during labor. Am J Obstet Gynecol 1994; 171: 993–8.
Gillberg C. “Floppy infant syndrome” and maternal diazepam (Letter). Lancet 1977; 2: 244.
Haram K. “Floppy infant syndrome” and maternal diazepam (Letter). Lancet 1977; 2: 612–3.
Dolovich LR, Addis A, Vaillancourt JM, Power JD, Koren G, Einarson TR. Benzodiazepine use in pregnancy and major malformations or oral cleft: metaanalysis of cohort and case-control studies. BMJ 1998; 317: 839–43.
Koren G, Pastuszak A, Ito S. Drugs in pregnancy. N Engl J Med 1998; 338: 1128–37.
Hoffmann AL, Hjortdal JO, Secher NJ, Weile B. The relationship between Apgar score, umbilical artery pH and operative delivery for fetal distress in 2778 infants born at term. Eur J Obstet Gynecol Reprod Biol 1990; 38: 97–101.
Socol ML, Garcia PM, Riter S. Depressed Apgar scores, acid-base status, and neurologic outcome. Am J Obstet Gynecol 1994; 170: 991–9.
Kuhnert BR, Linn PL, Kuhnert PM. Obstetric medication and neonatal behavior. Current controversies. Clin Perinatol 1985; 12:423–40.
Benlabed M, Dreizzen E, Ecoffey C, Escourrou P, Migdal M, Gaultier C. Neonatal patterns of breathing after cesarean section with or without epidural fentanyl. Anesthesiology 1990; 73: 1110–3.
Amiel-Tison C, Barrier G, Shnider SM, Levinson G, Hughes SC, Stefani SJ. The neonatal neurologic and adaptive capacity score (NACS) (Letter). Anesthesiology 1982; 56: 492–3.
Scanlon JW, Ostheimer GW, Lurie AO, Brown WUJr,Weiss JB, Alper MH. Neurobehavioral responses and drug concentrations in newborns after maternal epidural anesthesia with bupivacaine. Anesthesiology 1976; 45: 400–5.
Brockhurst NJ, Littleford JA, Halpern SH. The Neurologic and Adaptive Capacity Score. A systematic review of its use in obstetric anesthesia research. Anesthesiology 2000; 92: 237–46.
Camann W, Brazelton TB. Use and abuse of neonatal neurobehavioral testing (Editorial). Anesthesiology 2000; 92: 3–5.
Shnider SM, Abboud TK, Artal R, Henriksen EH, Stefani SJ, Levinson G. Maternal catecholamines decrease during labor after lumbar epidural anesthesia. Am J Obstet Gynecol 1983; 147: 13–5.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
A.Frölich, M., Burchfield, D.J., Euliano, T. et al. A single dose of fentanyl and midazolam prior to Cesarean section have no adverse neontal effects. Can J Anesth 53, 79–85 (2006). https://doi.org/10.1007/BF03021531
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03021531