
Abstract
Purpose
Median nerve somatosensory evoked responses (MnSSER) alterations were compared to clinical tests (cold and pinprick) variations, in 20 ASA I adult patients following infraclavicular block obtained with 40 mL ropivacaine 0.5% to assess first, the difference of time course of the respective electrophysiological and clinical signs, and second, the objectivity and the reproducibility of MnSSER changes.
Clinical features
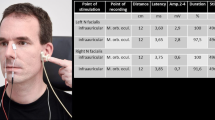
Four MnSSER derivations (Erb’s point; cutaneous projection of peripheral end of brachial plexus; posterior neck at C6 level, frontal and controlateral parietal scalp) were monitored and recorded for retrospective analysis. Continuous data acquisition were started before ropivacaine injection (baseline) and maintained for 30 min thereafter. Every three minutes after ropivacaine injection, cold and pinprick tests were performed in the hand median nerve cutaneous supply zone and were assessed using a sensory visual score (varying from 0–10). Data were compared using analysis of variance. Although MnSSER values were stable during baseline period, after ropivacaine administration, severe progressive amplitude depressions of selected MnSSER were detected in every patient. While clinical cold and pinprick tests became positive (score > 8) only 15.8 ± 1.2 min and 20.1 ± 1.8 min respectively after ropivacaine administration, the mean time to observe the earliest MnSSER 20% amplitude decrease at Erb’s point derivation was reduced to 5.6 ± 1.1 min (P < 0.01).
Conclusion
Selected MnSSER amplitude reduction indicates objectively the onset of median nerve anesthesia following infraclavicular brachial plexus block before the appearance of clinical signs.
Résumé
Objectif
Les modifications des potentiels évoqués somesthésiques du nerf médian (PESNM) induit par un block infraclaviculaire (40 mL de ropivacaine 0,5 %) on été comparés avec les tests cliniques usuels (tests au froid et à la piqûre) chez 20 patients adultes ASA I afin ďévaluer la différence ďévolution et de survenue des signes électrophysiologiques et cliniques, ľobjectivité et la reproductibilité des modifications des PESNM et finalement le possible intérêt en pratique clinique.
Eléments cliniques
Les PESMN étaient enregistrés en continu au point ďErb (projection cutanée de ľextrémité latérale du plexus brachial) et successivement au niveau cervical en regard de la sixime vertèbre), frontal et pariétal controlatéral pour une comparaison secondaire. Ľenregistrement a commencé avant ľinjection de ropivacaine et jusqu’à 30 min après. Toutes les trois minutes après la réalisation du bloc, les tests cliniques étaient réalisés au niveau de la main ďinnervation du nerf médian en utilisant une échelle visuelle analogique (0–10). Une analyse de variance a été utilisée pour comparer les résultats. Si les PESNM étaient remarquablement stables avant la réalisation du bloc, après leur amplitude diminue précocement et de fa÷on importante, chez tous les sujets. Alors que les tests au froid et à la piqûre peuvent être considérés comme positifs (> 8 sur ľéchelle) seulement après 15,8 ± 1,2 min et 20,1 ± 1,8 min respectivement après ľinjection de ropivacaêne, la diminution la plus précocement détectable de ľamplitude du potentiel (20 %) au point ďErb, survenait en moyenne en 5,6 ± 1,1 min (P < 0,01).
Conclusion
La diminution de ľamplitude des PESNM indique objectivement la survenue du bloc du nerf médian après la réalisation ďun bloc infraclaviculaire avant toute modification clinique.
Article PDF
Similar content being viewed by others


Avoid common mistakes on your manuscript.
References
Curatolo M, Petersen-Felix S, Arendt-Nielsen L. Sensory assessment of regional analgesia in humans: a review of methods and applications. Anesthesiology 2000; 93: 1517–30.
Paqueron X, Gentili ME, Willer JC, Coriat P, Riou B. Time sequence of sensory changes after upper extremity block: swelling sensation is an early and accurate predictor of success. Anesthesiology 2004; 101: 162–8.
Benzon HT, Toleikis JR, Shanks C, Ramseur A, Sloan T. Somatosensory evoked potential quantification of ulnar nerve blockade. Anesth Analg 1986; 65: 843–8.
Richardson J, Jones J, Atkinson R. The effect of thoracic paravertebral blockade on intercostal somatosensory evoked potentials. Anesth Analg 1998; 87: 373–6.
Murphy BA, Hvik Taylor H, Wilson SA, Knight JA, Mathers KM, Schug S. Changes in median nerve soamtosensory transmission and motor output following transient deafferentation of the radial nerve in humans. Clin Neurophysiol 2003; 114: 1477–88.
Weiss T, Miltner WH, Liepert J, Meissner W, Taub E. Rapid functional plasticity in the primary somatomotor cortex and perceptual changes after nerve block. Eur J Neurosci 2004; 20: 3413–23.
Lang E, Erdmann K, Gerbershagen HU. Median nerve blockade during diagnostic intravenous regional anesthesia as measured by somatosensory evoked potentials. Anesth Analg 1993; 76: 118–22.
Benzon HT, Toleikis JR, Dixit P, Goodman I, Hill JA. Onset, intensity of blockade and somatosensory evoked potential changes of the lumbosacral dermatomes after epidural anesthesia with alkalinized lidocaine. Anesth Analg 1993; 76: 328–32.
Raj PP, Montgomery SJ, Nettles D, Jenkins MT. Infraclavicular brachial plexus block - a new approach. Anesth Analg 1973; 52: 897–904.
Borene SC, Edwards JN, Boezrt AP. At the cords, the pinkie towards: interpreting infraclavicular motor responses to neurostimulation. Reg Anesth Pain Med 2004; 29: 125–9.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Pandin, P., Salengros, J.C., ďHollander, A. et al. Somatosensory evoked potentials as an objective assessment of the sensory median nerve blockade after infraclavicular block. Can J Anesth 53, 67–72 (2006). https://doi.org/10.1007/BF03021529
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03021529