
Abstract
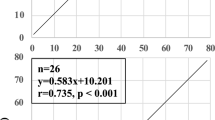
To determine the fresh gas flow (FGF) requirements in paediatric patients, we measured the FGFs needed to maintain distal end-tidal PCO2 (PetCO2) values at 30 and 38 mmHg in patients weighing between 3.8 and 20 kg ventilated with either a Sechrist Infant Ventilator IV-100B® or an Air-Shields Ventimeter® and a Mapleson D circuit. The FCF requirement was 500 ml·kg-1·min-1 to maintain a PetCO2 of 30 mmHg and 250 ml·kg-1·min-1 to maintain a PetCO2 of 38 mmHg when minute ventilation ≥ FGF. When these formulae were used in a subsequent group of similar patients, a wide variation in PetCO2 measurements were obtained. We conclude that the safest and most accurate approach to determine the FGF requirement of paediatric patients is to continuously monitor the PetCO2 in each patient and to adjust the FGF accordingly.
Résumé
Afin de déterminer la quantité de gas frais (FGF) requise en pédiatrie, on a mesuré les FGFs nécessaires afin de maintenir une PCO2 enfin ďexpiration (PetCO2) entre 30 et 38 mmHg chez des patients pesant entre 3.8 et 20 kg ventilés soit avec le ventilateur pédiatrique Sechrist IV 100B® ou un Air-Shields Ventimeter® et un circuit Mapleson D. Le FGF était de 500 ml·kg-1·min-1 afin de maintenir une PetCO2 à 30 mmHg et 250 ml·kg-1·min-1 afin de maintenir une PetCO2 de 38 mmHg quand la ventilation minute était ≥ au FGF. Quand ces formules ont été utilisées subséquemment pour un groupe similaire de patients une grande variation dans la mesure de la PetCO2 fut obtenue. On conclut que ľapproche la plus sécuritaire est la plus exacte afin de déterminer le FGF chez les patients pédiatriques est de continuer à surveiller la PetCO2 chez chaque patient et ďajuster la FGF en conséquence.
Article PDF
Similar content being viewed by others

Avoid common mistakes on your manuscript.
References
Ayre P. Anaesthesia for intracranial operation. Anew technique. Lancet 1937; 1: 561–3.
Rees GJ. Anaesthesia in the newborn. Br Med J 1950; 2: 1419–22.
Nightingale DA, Richards CC, Glass A. An evaluation of rebreathing in a modified t-piece system during controlled ventilation in anaesthetized children. Br J Anaesth 1965; 37: 762–70.
Hatch DJ, Yates AP, Lindahl SGE. Flow requirements and rebreathing during mechanically controlled ventilation in a T-piece (Mapleson E) system. Br J Anaesth 1987; 59: 1533–40.
Bain JA, Spoerel WE. Carbon dioxide output and elimination in children under anaesthesia. Can Anaesth Soc J 1977; 24: 533–9.
Rayburn RL, Graves SA, A new concept in controlled ventilation of children with the Bain anesthetic circuit. Anesthesiology 1978; 48: 250–3.
Rose DK, Froese AB. The regulation of PaCO2 during controlled ventilation of children with a t-piece. Can Anaesth Soc J 1979; 26: 104–13.
Badgwell JM, McLeod ME, Lerman J, Creighton RE. End-tidal PCO2 measurements sampled at the distal and proximal ends of the endotracheal tube in infants and children. Anesth Analg 1987; 66: 959–64.
Wolf AR, Volgysi GA. A modified Pitot tube for the accurate measurement of tidal volume in children. Anesthesiology 1987; 67: 775–8.
Badgwell JM,McLeod ME,Lerman J,Creighton RE. The accuracy of end-tidal PCO2 measurement in children ventilated with the Sechrist Infant Ventilator. Can J Anaesth, In press.
Badgwell JM, Heavner JE.May WS, Goldthorn JF, Lerman J. End-tidal PCO2 monitoring in infants and children ventilated with either a partial rebreathing or a non-rebreathing circuit. Anesthesiology 1987; 66: 405–10.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Badgwell, J.M., Wolf, A.R., McEvedy, B.A.B. et al. Fresh gas formulae do not accurately predict end-tidal PCO2 in paediatric patients. Can J Anaesth 35, 581–586 (1988). https://doi.org/10.1007/BF03020344
Issue Date:
DOI: https://doi.org/10.1007/BF03020344