
Abstract
Purpose
To establish the appropriate inhalation induction technique using a high concentration of sevoflurane in the elderly.
Methods
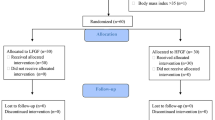
Forty-five patients, aged 70–79-yr-old, were randomly divided into three groups: 1) Group I: anesthesia was induced with propofol 2 mg·kg−1 and sevoflurane 2% (n = 15); 2) Group II: anesthesia was induced with a threeminute inhalation of sevoflurane 8%; 3) Group III: anesthesia was induced with inhalation of sevoflurane using a gradual reduction technique (8, 6, 4% for each minute). In Groups II and III, a modified vital capacity inhalation induction was performed. Mean arterial pressure (MAP), heart rate (HR) and oxygen saturation (SpO2) were measured continuously during induction. In addition, induction time and adverse events related to anesthetic induction were recorded.
Results
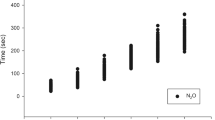
The induction time in Group I was significantly shorter than that in Groups II and III (P < 0.05). However, there was no difference in the induction time between Groups II and III. In Groups II and III, the majority of patients required additional breaths. In comparison with the other groups, stability of MAP was maintained in Group III. The variations of HR in all groups were small. During induction, no patient experienced a decrease in SpO2 below 96%, except for two patients in Group I. Severe respiratory adverse events were not observed. Other adverse events were similar in all groups.
Conclusions
Our results suggest that a high concentration sevoflurane induction using a gradual reduction technique may be an acceptable alternative to standard iv induction in elderly patients.
Résumé
Objectif
Réaliser la technique appropriée d’induction par inhalation en utilisant une forte concentration de sévoflurane chez des patients âgés.
Méthode
Quarante-cinq patients de 70–79 ans, ont été répartis de façon aléatoire en trois groupes : 1) groupe I : anesthésie induite avec 2 mg·kg−1 de propofol et du sévoflurane à2%(n = 15) ; 2) groupe II : anesthésie induite avec l’inhalation de sévoflurane à 8 % pendant 3 min ; 3) groupe III : anesthésie induite avec l’inhalation de sévoflurane selon la technique de réduction graduelle de la concentration (8, 6, 4 % pour chaque minute). Dans les groupes II et III, une induction par inhalation, avec modification de la capacité vitale, a été réalisée. La tension artérielle moyenne (TAM), la fréquence cardiaque (FR) et la saturation du sang en oxygène (SpO2) ont été mesurées en continu pendant l’induction. De plus, le temps nécessaire à l’induction et les événements indésirables reliés à l’induction anesthésique ont été notés.
Résultats
Le temps d’induction a été significativement plus court dans le groupe I que dans les groupes II et III (P < 0,05). Aucune différence de temps d’induction n’a été relevée entre les groupes II et III. Dans ces groupes II et III, la majorité des patients ont eu besoin de ventilation supplémentaire. Comparativement aux autres groupes, la stabilité de la TAM a été maintenue dans le groupe III. Les variations de FC ont été faibles dans tous les groupes. Pendant l’induction, aucun patient n’a subi de baisse de la SpO2 en dessous de 96 %, sauf deux patients du groupe I. Aucune complication respiratoire sévère n’a été observée. Les autres événements indésirables ont été comparables d’un groupe à l’autre.
Conclusion
Nos résultats montrent qu’une induction avec une forte concentration de sévoflurane, selon une technique de réduction graduelle, peut remplacer l’induction iv habituelle de façon acceptable chez les patients âgés.
Article PDF
Similar content being viewed by others

References
Yurino M, Kimura H. Vital capacity breath technique for rapid anaesthetic induction: comparison of sevoflruane and isoflurane. Anaesthesia 1992; 47: 946–9.
Yurino M, Kimura H. Vital capacity rapid inhalation induction technique: comparison of sevoflurane and halothane. Can J Anaesth 1993; 40: 440–3.
Hall JE, Oldham TA, Stewart JIM, Harmer M. Comparison between halothane and sevoflurane for adult vital capacity induction. Br J Anaesth 1997; 79: 285–8.
Yurino M, Kimura H. Induction of anesthesia with sevoflurane, nitrous oxide, and oxygen: a comparison of spontaneous ventilation and vital capacity rapid inhalation induction (VCRII) techniques. Anesth Analg 1993; 76: 598–601.
Philip BK, Lombard LL, Roaf ER, Drager LR, Calalang I, Philip JH. Comparison of vital capacity induction with sevoflurane to intravenous induction with propofol for adult ambulatory anesthesia. Anesth Analg 1999; 89: 623–7.
Thwaites A, Edmends S, Smith I. Inhalation induction with sevoflurane: a double-blind comparison with propofol. Br J Anaesth 1997; 78: 356–61.
Nishiyama T, Aibiki M, Hanaoka K. Haemodynamic and catecholamine changes during rapid sevoflurane induction with tidal volume breathing. Can J Anaesth 1997; 44: 1066–70.
Ti LK, Chow MYH, Lee TL. Comparison of sevoflurane with propofol for laryngeal mask airway insertion in adults. Anesth Analg 1999; 88: 908–12.
Yamaguchi S, Egawa H, Okuda K, Mishio M, Okuda Y, Kitajima T. High concentration sevoflurane induction of anesthesia accelerates onset of vecuronium neuromuscular blockade. Can J Anesth 2001; 48: 34–7.
Walpole R, Logan M. Effect of sevoflurane concentration on inhalation induction of anaesthesia in the elderly. Br J Anaesth 1999; 82: 20–4.
Jin F, Chung F. Minimizing perioperative adverse events in the elderly. Br J Anaesth 2001; 87: 608–24.
Nakajima R, Nakajima Y, Ikeda K. Minimum alveolar concentration of sevoflurane in elderly patients. Br J Anaesth 1993; 70: 273–5.
Mapleson WW. Effect of age on MAC in humans: a meta-analysis. Br J Anaesth 1996; 76: 179–85.
Mangano DT. Perioperative cardiac morbidity. Anesthesiology 1990; 72: 153–84.
Mangano DT, Browner WS, Hollenberg M, London MJ, TubauJF, Tateo IM. Association of perioperative myocardial ischemia with cardiac morbidity and mortality in men undergoing noncardiac surgery. The Study of Perioperative Ischemia Research Group. N Engl J Med 1990; 323: 1781–8.
Slogoff S, Keats AS. Does perioperative myocardial ischemia lead to postoperative myocardial infarction? Anesthesiology 1985; 62: 107–14.
Nathan N, Vial G, Benrhaiem M, Peyclit A, FeissP. Induction with propofol taget-concentration infusion vs. 8% sevoflurane inhalation and alfentanil in hypertensive patients. Anaesthesia 2001; 56: 248–71.
Cheong KF, Choy JML. Sevoflurane-fentanyl versus etomidate-fentanyl for anesthetic induction in coronary artery bypass graft surgery patients. J Cardiothor Vasc Anesth 2000; 14: 421–4.
Gravel NR, Searle NR, Taillefer J, Carrier M, Roy M, Gagnon L. Comparison of the hemodynamic effects of sevoflurane anesthesia induction and maintenance vs TIVA in CABG surgery. Can J Anesth 1999; 46: 240–6.
Djaiani GN, Hall J, Pugh S, Peaston RT. Vital capacity inhalation induction with sevoflurane: an alternative to standard intravenous induction for patients undergoing cardiac surgery. J Cardiothor Vasc Anesth 2001; 15: 169–74.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Yamaguchi, S., Ikeda, T., Wake, K. et al. A sevoflurane induction of anesthesia with gradual reduction of concentration is well tolerated in elderly patients. Can J Anesth 50, 26–31 (2003). https://doi.org/10.1007/BF03020182
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03020182