
Abstract
Purpose
Following ambulatory surgery, long-acting analgesics may provide advantages over short-acting analgesics. This study compared controlled-release codeine (CC) and acetaminophen plus codeine (A/C; 300 mg/30 mg) for pain control in the 48-hr period following laparoscopic cholecystectomy
Methods
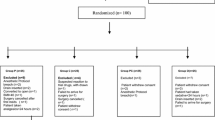
Eligible patients were randomized to CC or A/C in a double-blind, double-dummy parallel group study. Unrelieved pain in hospital was treated with fentanyliv bolus. Rain [100 mm visual analogue scale (VAS)] was assessed before the first dose of medication; at 0.5, one, two, three, and four hours post-dose; at discharge; and three times a day for 48 hr. Adverse events were recorded and measures of patient satisfaction were assessed at the end of the study.
Results
Eighty-four patients were enrolled in the study; 42 patients in each group. There were no statistically significant differences between CC and A/C treatment. Mean VAS baseline pain was similar in both groups (P = 0.49) and there was no significant difference in the time to onset of analgesia (P = 0.17). At 0.5 hr, the mean VAS pain score was significantly reduced from baseline in both groups (P = 0.0001). The VAS pain scores at discharge were reduced 59% and 56% from baseline, respectively (P = 0.61). There was no difference between treatments in the incidence of adverse events and patients reported similar levels of satisfaction.
Conclusions
Controlled-release codeine provides an equivalent onset of analgesia, reduction in postoperative pain, and level of patient satisfaction, to acetaminophen plus codeine, over 48 hr following cholecystectomy, with the advantage of less frequent dosing.
Résumé
Objectif
En chirurgie ambulatoire, les analgésiques postopératoires d’action prolongée peuvent avoir des avantages sur les analgésiques d’action brève. Nous comparons la codéine à libération contrôlée (CC) et une combinaison d’acétaminophène et de codéine (A/C; 300 mg/30 mg) comme analgésique pendant 48 h après une cholécystectomie laparoscopique.
Méthode
Des patients admissibles à l’expérimentation ont reçu de la CC ou de l’A/C lors d’une étude à double insu, à double placebo en contrôle parallèle. A l’hôpital, la douleur tenace a été traitée avec des bolus iv de fentanyl. La douleur [échelle visuelle analogique (EVA) de 100 mm] a été évaluée avant la première dose de médicament; à 0,5, une, deux, trois et quatre heures après la dose; au moment du départ et trois fois par pur pendant 48 h. Les événements indésirables ont été notés et des mesures de la satisfaction du patient ont été faites à la fin de l’étude.
Résultats
Létude a été réalisée auprès de 84 patients: 42 dans chaque groupe. Il n’y a pas eu de différence statistiquement significative entre les traitements à la CC ou à l’A/C. La douleur initiale moyenne a été similaire dans les deux groupes (P = 0,49) et il n’y a pas eu de différence significative de temps précédant le début de l’analgésie (P = 0,17). À 0,5 h, le score de douleur moyen à l’EVA était significativement réduit dans les deux groupes (P = 0,0001). Les scores à l’EVA au départ de l’hôpital ont été respectivement réduits de 59 % et de 56 % par rapport aux mesures initiales de la douleur (P = 0,61). Aucune différence intergroupe dans l’incidence d’événements indésirables n’a été notée et la satisfaction des patients était comparable d’un groupe à l’autre.
Conclusion
La codéine à libération contrôlée offre un délai d’installation de l’analgésie, une réduction de la douleur postopératoire et un niveau de satisfaction équivalents à une combinaison d’acétaminophène et de codéine pendant 48 h après une cholécystectomie, et ce, avec l’avantage d’un dosage moins fréquent.
Article PDF
Similar content being viewed by others


References
Cuschieri A. Laparoscopic cholecystectomy: indications, technique and results, pros and cons. Dig Surg 1991; 8: 104–7.
Jakimowicz JJ. Cholecystectomy — the ‘golden standard’ treatment for cholecystolithiasis: the evolution of surgical technique. Dig Surg 1991; 8: 71–5.
Hospital Morbidity Database, Canadian Institute for Health Information (CIHI). Ontario Ministry of Health, 2002.
Anonymous. A prospective analysis of 1518 laparoscopic cholecystectomies. The Southern Surgeons Club. N Engl J Med 1991; 324: 1073–8.
Berci G, Sackier JM. The Los Angeles experience with laparoscopic cholecystectomy. Am J Surg 1991; 161: 382–4.
Michaloliakou C, Chung F, Sharma S. Preoperative multimodal analgesia facilitates recovery after ambulatory laparoscopic cholecystectomy. Anesth Analg 1996; 82: 44–51.
Joshi GP. Postoperative pain management. Int Anesthesiol Clin 1994; 32: 113–26.
Joris J, Thiry E, Paris P, Weerts J, Lamy M. Pain after laparoscopic cholecystectomy: characteristics and effect of intraperitoneal bupivacaine. Anesth Analg 1995; 81: 379–84.
Joris J, Cigarini I, Legrand M, et al. Metabolic and respiratory changes after cholecystectomy performed via laparotomy or laparoscopy. Br J Anaesth 1992; 69: 341–5.
Collins KM, Docherty PW, Plantevin OM. Postoperative morbidity following gynaecological outpatient laparoscopy. A reappraisal of the service. Anaesthesia 1984; 39: 819–22.
Edwards ND, Barclay K, Catling SJ, Martin DG, Morgan RH. Day case laparoscopy: a survey of postoperative pain and an assessment of the value of diclofenac. Anaesthesia 1991; 46: 1077–80.
Graf DE, Pandit SK, Kothary SP, Ereeland GR. A double-blind comparison of orally administered ciramadol and codeine for relief of postoperative pain. J Clin Pharmacol 1985; 25: 590–5.
Brunette RL, George RE, Sunshine A, Hammonds WD. Analgesic effect of picenadol, codeine, and placebo in patients with postoperative pain. Clin Pharmacol Ther 1988; 43: 663–7.
Gertzbein SD, Tile M, McMurty RY, et al. Analysis of the analgesic efficacy of acetaminophen 1000 mg, codeine phosphate 60 mg, and the combination of acetaminophen 1000 mg and codeine phosphate 60 mg in the relief of postoperative pain. Pharmacotherapy 1986; 6: 104–7.
Forbes JA, Bates JA, Edquist IA, et al. Evaluation of two opioid-acetaminophen combinations and placebo in postoperative oral surgery pain. Pharmacotherapy 1994; 14: 139–46.
Acute Pain Management Guideline Panel. Acute Pain Management: Operative or Medical Procedures and Trauma. Clinical Practice Guidelines. AHCPR Pub No. 92-0032, Rockville, MD: Agency for Health Care Policy and Research, Public Health Service. U.S. Department of Health and Human Services. February 1992.
Narchi P, Benhamou D, Fernandez H. Intraperitoneal local anaesthetic for shoulder pain after day-case laparoscopy. Lancet 1991; 338: 1569–70.
Riedel HH, Semm K. The post-laparoscopic pain syndrome (author’s syndrome) (German). Geburtshilfe Frauenheilkd 1980; 40: 635–43.
Beauregard L, Pomp A, Choiniere M. Severity and impact of pain after day-surgery. Can J Anaesth 1998; 45: 304–11.
Reuben SS, Connelly NR, Maciolek H. Postoperative analgesia with controlled-release oxycodone for outpatient anterior cruciate ligament surgery. Anesth Analg 1999; 88: 1286–91.
Band CJ, Band PR, Deschamps M, Besner JG, Coldman AJ. Human pharmacokinetic study of immediate-release (codeine phosphate) and sustained-release (Codeine Contin) codeine. J Clin Pharmacol 1994; 34: 938–43.
Aldrete JA, Kroulik D. A postanesthetic recovery score. Anesth Analg 1970; 49: 924–34.
Aldrete JA. The post-anesthesia recovery score revisited (Letter). J Clin Anesth 1995; 7: 89–91.
Cleeland CS, Ryan KM. Pain assessment: global use of the brief pain inventory. Ann Acad Med Singapore 1994; 23: 129–38.
Kinnard P, Lirette R. Outpatient orthopedic surgery: a retrospective study of 1996 patients. Can J Surg 1991; 34: 363–6.
Fortier J, Chung F, Su J. Unanticipated admission after ambulatory surgery: a prospective study. Can J Anaesth 1998; 45: 612–9.
Jin EL, Chung F. Postoperative pain — a challenge for anaesthetists in ambulatory surgery. Can J Anaesth 1998; 45: 293–6.
Bisgaard T, Klarskov B, Rosenberg J, Kehlet H. Factors determining convalescence after uncomplicated laparoscopic cholecystectoymy. Arch Surg 2001; 136; 917–21.
Sunshine A, Olson NZ, Colon A, et al. Analgesic efficacy of controlled-release oxycodone in postoperative pain. J Clin Pharmacol 1996; 36: 595–603.
Mandema JW, Kaiko RF, Oshlack B, Reder RF, Stanski DR. Characterization and validation of a pharmacokinetic model for controlled-release oxycodone. Br J Clin Pharmacol 1996; 42: 747–56.
Crews JC. Multimodal pain management strategies for office-based and ambulatory procedures. JAMA 2002; 288: 629–32.
Author information
Authors and Affiliations
Corresponding author
Additional information
This study was partially supported by a grant from Purdue Pharma (Canada) Inc.
Rights and permissions
About this article
Cite this article
Chung, F., Tong, D., Miceli, P.C. et al. Controlled-release codeine is equivalent to acetaminophen plus codeine for post-cholecystectomy analgesia. Can J Anesth 51, 216–221 (2004). https://doi.org/10.1007/BF03019098
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03019098