
Abstract
Purpose
To describe a patient diagnosed with pheochromocytoma in the third trimester of pregnancy and discuss the perioperative and anesthetic management.
Clinical features
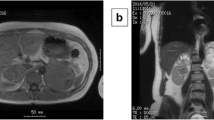
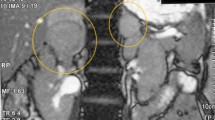
A 32-yr-old previously healthy woman (gravida 4, para 2) presented to our tertiary care obstetrical hospital at 34 weeks five days gestation with a history of labile blood pressure and severe hypertension. A week prior to admission she began having episodes of severe headache, dizziness, sweating and nausea. On a routine obstetric visit she was noted to be severely hypertensive with a blood pressure of 200/120 mmHg. Biochemical investigations confirmed the diagnosis of pheochromocytoma and magnetic resonance imaging demonstrated a 3 cm × 3 cm right adrenal mass. The patient was invasively monitored in the intensive care unit and treated with alpha-followed by beta-blockade with phenoxybenzamine and metoprolol. A multidisciplinary conference was organized involving endocrinology, anesthesiology, general surgery and obstetrics to determine the most appropriate management of the patient. An uncomplicated laparoscopic adrenalectomy was performed following a period of recovery after an uneventful elective Cesarean delivery.
Conclusions
The primary goals in the management of pheochromocytoma in pregnancy are early diagnosis, avoidance of a hypertensive crisis during delivery and definitive surgical treatment. Timing of surgical resection will depend on the gestational age at which diagnosis is made. Cesarean section is the preferred mode of delivery when the tumour is still present. This case illustrates that with antenatal diagnosis, advanced methods of tumour localization, adequate preoperative adrenergic blockade and team planning, pheochromocytoma in pregnancy can be treated successfully.
Résumé
Objectif
Présenter une patiente chez qui on a découvert un phéochromocytome au troisième trimestre de la grossesse, et son traitement périopératoire et anesthésique.
Éléments cliniques
Une femme de 32 ans, antérieurement en bonne santé (G4, P2) s’est présentée à notre hôpital obstétrical de soins tertiaires à 34 semaines et cinq jours de grossesse. Elle avait une histoire de tension artérielle labile et de sévère hypertension. Une semaine avant l’hospitalisation, elle a eu des épisodes de céphalées sévères, étourdissements, transpiration et nausées. Lors d’une visite obstétricale de routine, une tension artérielle de 200/120 mmHg avait indiqué une hypertension importante. Les examens biochimiques ont confirmé le diagnostic de phéochromocytome et l’imagerie par résonance magnétique a montré une masse surrénalienne droite de 3 cm × 3 cm. La patiente, sous monitorage effractifà l’unité des soins intensifs, a reçu des alpha-bloqueurs, puis des bêta-bloqueurs combinés à de la phénoxybenzamine et à du métoprolol. Une réunion des endocrinologue, anesthésiologiste, chirurgien général et obstétricien a permis de déterminer le traitement le plus approprié. Une surrénalectomie laparoscopique sans complications a été exécutée après que la patiente a été remise de la césarienne sans incident réalisée auparavant.
Conclusions
Le traitement d’un phéochromocytome pendant la grossesse visent à établir un diagnostic précoce, à empêcher une crise hypertensive pendant l’accouchement et à procéder à l’intervention chirurgicale définitive. Le moment choisi pour la résection dépend de l’âge gestationnel au moment du diagnostic. La césarienne est le mode d’accouchement privilégié lorsque la tumeur est toujours présente. Le cas présent montre que le diagnostic prénatal, des méthodes perfectionnées de localisation de la tumeur, un bloc adrénergique préopératoire adéquat et une planification multidisciplinaire permettent de traiter avec succès un phéochromocytome pendant la grossesse.
Article PDF
Similar content being viewed by others

References
Wissler RN. Endocrine disorders. In: Chestnut DH (Ed.). Obstretric Anesthesia. Principles and Practice, 2nd ed. New York: Mosby Year Book Inc.; 1999: 828–32.
Lau P, Permezel M, Dawson P, Chester S, Collier N, Forbes I. Phaeochromocytoma in pregnancy. Aust NZ J Obstet Gynaecol 1996; 36: 472–6.
Freier DT, Thompson NW. Pheochromocytoma and pregnancy: the epitome of high risk. Surgery 1993; 114: 1148–52.
Mastrogiannis DS, Whiteman VE, Mamopoulos M, Salameh WA. Acute endocrinopathies during pregnancy. Clin Obstet Gynecol 1994; 37: 78–92.
Harrington JL, Farley DR, van Heerden JA, Ramin KD. Adrenal tumors and pregnancy. World J Surg 1999; 23: 182–6.
Harper MA, Murnaghan GA, Kennedy L, Hadden DR, Atkinson AB. Phaeochromocytoma in pregnancy. Five cases and a review of the literature. Br J Obstet Gynaecol 1989; 96: 594–606.
Stoelting RK, Dierdorf SF. Anesthesia and Co-Existing Disease, 4th ed. New York: Churchill Livingstone Inc.; 2002: 430–4.
Bullough AS, Karadia S, Watters M. Phaeochromocytoma: an unusual cause of hypertension in pregnancy. Anaesthesia 2001; 56: 43–6.
Almog B, Kupferminc MJ, Many A, Lessing JB. Pheochromocytoma in pregnancy —a case report and review of the literature. Acta Obstet Gynecol Scand 2000; 79: 709–11.
Inabnet WB, Pitre J, Bernard D, Chapuis Y. Comparison of the hemodynamic parameters of open and laparoscopic adrenalectomy for pheochromocytoma. World J Surg 2000; 24: 574–8.
Gagner M, Lacroix A, Prinz RA, et al. Early experience with laparoscopic approach for adrenalectomy. Surgery 1993; 114: 1120–5.
Schenker JG, Granat M. Phaeochromocytoma and pregnancy-an updated appraisal. Aust NZ J Obstet Gynaecol 1982; 22: 1–10.
O’Riordan JA. Pheochromocytomas and anesthesia. Int Anesthesiol Clin 1997; 35: 99–127.
James MF, Huddle KR, Owen AD, van der Veen BW. Use of magnesium sulphate in the anaesthetic management of phaeochromocytoma in pregnancy. Can J Anaesth 1988; 35: 178–82.
Pullerits J, Ein S, Balfe JW. Anaesthesia for phaeochromocytoma. Can J Anaesth 1988; 35: 526–34.
Stonham J, Wakefield C. Phaeochromocytoma in pregnancy. Caesarean section under epidural analgesia. Anaesthesia 1983; 38: 654–8.
Santeiro ML, Stromquist C, Wyble L. Phenoxybenzamine placental transfer during the third trimester. Ann Pharmacother 1996; 30: 1249–51.
Kan RE, Hughes SC, Rosen MA, Kessin C, Preston PG, Lobo EP. Intravenous remifentanil. Placental transfer, maternal and neonatal effects. Anesthesiology 1998; 88: 1467–74.
Janetschek G, Neumann HP. Laparoscopic surgery for pheochromocytoma. Urol Clin North Am 2001; 28: 97–105.
Fernandez-Cruz L, Taura P, Saenz A, Benarroch G, Sabater L. Laparoscopic approach to pheochromocytoma: hemodynamic changes and catecholamine secretion. World J Surg 1996; 20: 762–8.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Dugas, G., Fuller, J., Singh, S. et al. Pheochromocytoma and pregnancy: a case report and review of anesthetic management. Can J Anesth 51, 134–138 (2004). https://doi.org/10.1007/BF03018772
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03018772