
Structured abstract
Question
Does daily intermittent hemodialysis improve survival as compared with conventional (alternate day) intermittent dialysis in patient with acute renal failure?
Design
Prospective, nonrandomized (alternating allocation), controlled trial. Patients, physicians and nursing staff were unaware of treatment assignment before the first dialysis but blinding was impossible thereafter.
Setting
Medical and surgical intensive care units in a single teaching hospital in Germany from January 1993 to September 1998.
Patients
One hundred and sixty adult patients with acute renal failure (ARF) from acute tubular necrosis were alternatively assigned to one of two treatment regimens. ARF was defined as a serum creatinine increase of at least 88 mmol · L−1 · day−1 or a value > 353 mmol · L−1. Exclusion criteria were chronic renal failure (serum creatinine > 265 mmol · L−1 ); other causes for acute renal failure (obstructive, interstitial nephritis, glomerulonephritis); previous renal transplantation; prior dialysis treatment; or treatment with continuous renal replacement therapy (CRRT).
Intervention
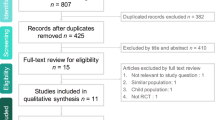
Eighty patients were allocated to each treatment arm. Fourteen patients were withdrawn during the course of the study. Seventy-four patients received daily dialysis (six days/week) and 72 patients received dialysis every other day (three days/week). The dose of hemodialysis was adjusted based on the basis of the urea kinetic formula (Kt/V) and pre-treatment body weight. Hemodialysis was stopped at partial recovery of renal function defined as a return of diuresis, absence of uremia and improved metabolic homeostasis as judged by the nephrologists, without specified values.
Main outcomes
Mortality from any cause 14 days after the last dialysis was the primary outcome. Frequency of treatment-related complication and the duration of renal failure were secondary outcomes.
Main results
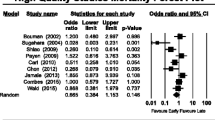
Analysis was by “intention-to-treat”. Baseline characteristics were similar in both groups including the etiology of renal failure, APACHE III score, serum creatinine, blood urea nitrogen and the percentage of patients with oliguria at entry. The daily dialysis group had 28% mortality compared to 46% in the conventional group with an absolute risk reduction of 18% and number-needed-to-treat of 6. There were fewer complications in the daily dialysis group and a shorter time to recovery from renal failure. The sample size was powered to detect a 20% difference in mortality.
Conclusion
Daily dialysis reduces all-cause mortality in patients with acute renal failure.
Funding
No source of external funding was mentioned.
Article PDF
Similar content being viewed by others

Avoid common mistakes on your manuscript.
References
Tonelli M, Manns B, Feller-Kopman D. Acute renal failure in the intensive care unit: a systematic review of the impact of dialytic modality on mortality and renal recovery. Am J Kidney Dis 2002; 40: 875–85.
Anonymous. NKF-DOQI clinical practice guidelines for hemodialysis adequacy. National Kidney Foundation. Am J Kidney Dis 1997; 30(3 Suppl 2): S15–66.
Ronco C, Bellomo R, Homel P, et al. Effects of different doses in continuous veno-venous haemofiltration on outcomes of acute renal failure: a prospective randomised trial. Lancet 2000; 356: 26–30.
Vanholder R, Van Biesen W, Lameire N. What is the renal replacement method of first choice for intensive care patients? J Am Soc Nephrol 2001; 12(Suppl 17): S40–3.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Bernard, F., Verdant, C.L., Gorman, T. et al. Best evidence in critical care medicine. Can J Anesth 50, 953–954 (2003). https://doi.org/10.1007/BF03018746
Issue Date:
DOI: https://doi.org/10.1007/BF03018746