
Abstract
Purpose
Intrathecal morphine and psoas compartment block represent two accepted techniques to provide postoperative analgesia after hip arthroplasty. We designed a prospective, randomized, single-blinded study to compare these two techniques.
Methods
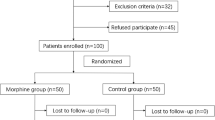
Patients scheduled for primary hip arthroplasty under general anesthesia were randomized to receive either an intrathecal administration of 0.1 mg morphine (Group I,n = 27) or a psoas compartment block with ropivacaine 0.475% 25 mL (Group II,n = 26). Pain scores, morphine consumption, associated side-effects were assessed for 48 hr postoperatively. In addition, patient’s acceptance and satisfaction of the postoperative analgesic technique were also recorded.
Results
During the first 24 hr, pain scores (3.3 ± 9.6 mm vs 22.8 ± 27.1 at H+6, 3.3 ± 8.3 mm vs 25 ± 26.7 mm at H+ 12, 7 ± 14.9 mm vs 21.9 ± 29 mm at H+18) and morphine consumption (0.56 ± 2.12 mg vs 9.42 ± 10.13 mg) were lower in Group I than in Group II. Urinary retention was the more frequent side-effect occurring in 37% of cases in Group I vs 11.5% in Group II (P < 0.05). No major complication occurred. Despite better analgesia provided by the use of intrathecal morphine, there was no difference in the satisfaction scores between groups.
Conclusion
0.1 mg intrathecal morphine administration provides better postoperative analgesia than single-shot psoas compartment block after primary hip arthroplasty.
Résumé
Objectif
La rachianalgésie morphinique et le bloc du plexus lombaire par voie postérieure sont deux techniques adéquates pour assurer l’analgésie postopératoire après la mise en place d’une prothèse totale de hanche. Dans cette étude, ces deux techniques sont comparées de manière prospective, randomisée et simple aveugle.
Méthode
Avant l’anesthésie générale, les patients étaient tirés au sort pour recevoir soit une injection intrathécale lombaire de 0,1 mg de morphine (Groupe I, n = 27), soit un bloc du plexus lombaire par voie postérieure avec injection unique de 25 mL de ropivacaïne à 0,475 % (Groupe II, n = 26). Les scores de douleur, la consommation de morphine et les effets secondaires étaient évalués pendant les 48 premières heures postopératoires. De plus, l’acceptation par le patient de la technique analgésique et sa satisfaction pour la prise en charge de la douleur postopératoire étaient également comparées.
Résultats
Dans les 24 premières heures, les scores de douleur (3,3 ± 9,6 mm vs 22,8 ±27,1 à H+6; 3,3 ± 8,3 mm vs 25 ± 26,7 mm à H+12; 7 ± 14,9 mm vs 21,9 ± 29 mm à H+18) et la consommation de morphine (0,56 ± 2,12 mg vs 9,42 ± 10,13 mg) étaient significativement moins élevés dans le Groupe I que dans le Groupe II. La rétention urinaire était plus fréquente dans le Groupe I (37 % vs 11,5 %). Aucune complication grave n’est survenue. En dépit d’une meilleure analgésie procurée par la rachianalgésie morphinique, la satisfaction était comparable dans les deux groupes.
Conclusion
La conclusion principale de cette étude est que la rachianalgésie morphinique procure une meilleure analgésie postopératoire que le bloc du plexus lombaire par voie postérieure en injection unique après la mise en place d’une prothèse totale de hanche.
Article PDF
Similar content being viewed by others

Avoid common mistakes on your manuscript.
References
Capdevilla X, Barthelet Y, Biboulet P, Ryckwaert Y, Rubenovitch J, d’Athis F. Effects of perioperative analgesic technique on the surgical outcome and duration of rehabilitation after major knee surgery. Anesthesiology 1999; 91: 8–15.
Chelly JE, Greger J, Gebhard R, et al. Continuous femoral blocks improve recovery and outcome of patients undergoing total knee arthroplasty. J Arthroplasty 2001; 16: 436–45.
Grace D, Fee JPH. A comparison of intrathecal morphine-6-glucuronide and intrathecal morphine sulfate as analgesics for total hip replacement. Anesth Analg 1996; 83: 1055–9.
Reay BA, Semple AJ, Macrae WA, MacKenzie N, Grant IS. Low-dose intrathecal diamorphine analgesia following major orthopaedic surgery. Br J Anaesth 1989; 62: 248–52.
Slappendel R, Weber EWG, Dirksen R, Gielen MJM, van Limbeek J. Optimization of the dose of intrathecal morphine in total hip surgery: a dose-finding study. Anesth Analg 1999; 88: 822–6.
Stevens RD, Van Gessel E, Flory N, Fournier R, Gamulin Z. Lumbar plexus block reduces pain and blood loss associated with total hip arthroplasty. Anesthesiology 2000; 93: 115–21.
Aida S, Takahashi H, Shimoji K. Renal subcapsular hematoma after lumbar plexus block. Anesthesiology 1996; 84: 452–5.
Klein SM, D’Ercole F, Greengrass RA, Warner DS. Enoxaparin associated with psoas hematoma and lumbar plexopathy after lumbar plexus block. Anesthesiology 1997; 87: 1576–9.
Gentili M, Aveline C, Bonnet F. Total spinal anesthesia after posterior lumbar plexus block (French). Ann Fr Anesth Réanim 1998; 17: 740–2.
Pham-Dang C, Beaumont S, Floch H, Bodin J, Winer A, Pinaud M. Acute toxic accident following lumbar plexus block with bupivacaine (French). Ann Fr Anesth Réanim 2000; 19: 356–9.
Winnie AP. Regional anesthesia. Surg Clin North Am 1975; 54: 861–92.
Testud L. Système Nerveux Périphériques, Organe des Sens, Appareil de la Respiration et de la Phonation. Traité d’Anatomie Humaine, tome 3. Lyon; 1922.
Chudinov A, Berkenstadt H, Salai M, Cahana A, Perel A. Continuous psoas compartment block for anesthesia and perioperative analgesia in patients for hip fractures. Reg Anesth Pain Med 1999; 24: 563–8.
Benedetti C, Bonica JJ, Belluci G. Pathophysiology and therapy of postoperative pain: a review.In: Benedetti C, Bonica JJ, Belluci G. (Eds.). Advances in Pain Research and Therapy, vol. 7. New York: Raven Press; 1984: 373–407.
Singelyn FJ, Vanderelst PE, Gouverneur JMA. Extended femoral nerve sheath block after total hip arthroplasty: continuous versus patient-controlled techniques. Anesth Analg 2001; 92: 455–9.
Capdevilla X, Macaire P, Dadure C, et al. Continuous psoas compartment block for postoperative analgesia after total hip arthroplasty: new landmarks, technical guidelines, and clinical evaluation. Anesth Analg 2002; 94: 1606–13.
Michelson JD, Lotke PA, Steinberg ME. Urinary-bladder management after total joint-replacement surgery. N Engl J Med 1988; 319: 321–6.
Kinirons BP, Bouaziz H, Paqueron X, et al. Sedation with sufentanil and midazolam decreases pain in patients undergoing upper limb surgery under multiple nerve block. Anesth Analg 2000; 90: 1118–21.
Koscielniak-Nielsen ZJ, Rassmussen H, Jepsen K. Effects of impulse duration on patients’ perception of electrical stimulation and block effectiveness during axillary block in unsedated ambulatory patients. Reg Anesth Pain Med 2001; 26: 428–33.
Fung D, Cohen MM. Measuring patient satisfaction with anesthesia care: a review of current methodology. Anesth Analg 1998; 87: 1089–98.
Wu CL, Naqibuddin M, Fleisher LA. Measurements of patient satisfaction as an outcome of regional anesthesia and analgesia: a systematic review. Reg Anesth Pain Med 2001; 26: 196–208.
Le May S, Hardy JF, Taillefer MC, Dupuis G. Patient satisfaction with anesthesia services. Can J Anesth 2001; 48: 153–62.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Souron, V., Delaunay, L. & Schifrine, P. Intrathecal morphine provides better postoperative analgesia than psoas compartment block after primary hip arthroplasty. Can J Anesth 50, 574–579 (2003). https://doi.org/10.1007/BF03018643
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03018643