
Abstract
Purpose
We compared the efficacy of epidural continual intermittent boluses (CIB) with a continuous epidural infusion (CEI) in prolonging labour analgesia induced by the combined spinal epidural (CSE) technique.
Methods
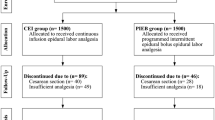
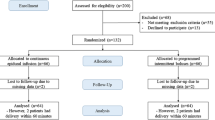
CSE was instituted in 42 nulliparous parturients at the L3 to 4 level with intrathecal (IT) fentanyl 25 μg followed by an epidural test dose of 3 mL of 1.5% lidocaine. These parturients were then randomly assigned to receive either epidural CIB (n = 21) or CEI (n = 21) with 0.1% ropivacaine and fentanyl 2 μg·mL−1. For the CIB, 5 mL boluses were given hourly, with the first bolus 30 min postinduction. CEI at the rate of 5 mL·hr−1 was initiated in the minute after CSE. The duration of analgesia, pain score, degree of sensorimotor block were compared.
Results
From Kaplan Meier survival analysis, the duration of analgesia was significantly longer in CIB (mean survival time 239 ± SD 24 min vs 181 ± 17,P < 0.05 using log rank test). During the first three hours postblock, the median sensory block to cold was higher in CIB (P < 0.05, Mann U Whitney test) but no difference in blood pressure was detected (P > 0.05, repeated measure analysis of variance (RMANOVA)]. The serial pain scores were lower in the CIB (P < 0.05, RMANOVA).
Conclusion
CIB prolonged the duration and improved the quality of analgesia. CIB could have resulted in an improved spread of analgesics in the epidural space or encouraged a direct passage of infusate into the IT space. This could have also rendered a higher sensory block to cold in the CIB group. CIB is a good alternative to CEI for the maintenance of epidural analgesia after CSE.
Résumé
Objectif
Comparer l’efficacité de bolus périduraux intermittents administrés en continu (BIC) avec la perfusion péridurale continue (PPC) comme analgésie prolongée pendant le travail induite selon une technique rachidienne péridurale combinée (RPC).
Méthode
L’analgésie RPC a été installée chez 42 parturientes nullipares au niveau L3 à 4 avec 25 μg de fentanyl intrathécal (IT) suivi d’une dose test péridurale de 3 mL de lidocaïne à 1,5 %. Les patientes ont été randomisées pour recevoir soit des BIC périduraux (n = 21), soit une PPC (n = 21) avec ropivacaïne à 0,1 % et 2 μg·mL−1 de fentanyl. Dans le cas des BIC, des bolus de 5 mLà chaque heure ont été donnés, dont le premier 30 min après l’induction. La PPC a débuté une minute après la RPC à raison de 5 mL·h−1. La durée de l’analgésie, les scores de douleur, le degré de bloc sensorimoteur ont été comparés.
Résultats
À partir de l’analyse de survie de Kaplan Meier, on a trouvé une analgésie significativement plus longue avec les BIC (temps de survie moyen de 239 ± l’écart type 24 min vs 181 ± 17, P < 0,05 avec le test du logrank). Pendant les trois premières heures suivant le bloc, le bloc sensitif moyen au froid a été plus élevé avec les BIC (P < 0,05, test U de Mann Whitney) mais aucune différence de tension artérielle n’a été détectée [P > 0,05, analyse répétée de la variance à plusieurs variables (repeated measure analysis of variance RMANOVA)]. Les scores de douleur en série ont été plus bas avec les BIC (P < 0,05, RMANOVA).
Conclusion
Les BIC ont prolongé la durée et amélioré la qualité de l’analgésie. Les BIC peuvent améliorer la diffusion de l’analgésie dans l’espace péridural ou favoriser le passage direct de la perfusion dans l’espace IT. Cette technique peut aussi avoir augmenté le bloc sensitif au froid. Les BIC sont un bon équivalent de la PPC pour le maintien de l’analgésie péridurale après la RPC.
Article PDF
Similar content being viewed by others

References
Gaiser RR, Lewin SB, Cheek TG, Gutsche BB. Effects of immediately initiating an epidural infusion in the combined spinal and epidural technique in nulliparous parturients. Reg Anesth Pain Med 2000; 25: 223–7.
Kaynar AM, Shankar KB. Epidural infusion: continuous or bolus? (Letter). Anesth Analg 1999; 89: 534.
Norris MC, Ferrenbach D, Dalman H, et al. Does epinephrine improve the diagnostic accuracy of aspiration during labor epidural analgesia? Anesth Analg 1999; 88: 1073–6.
Beilin Y, Nair A, Arnold I, et al. A comparison of epidural infusions in combined spinal/ epidural technique for labor analgesia. Anesth Analg 2002; 94: 927–32.
Hogan Q. Distribution of solution in the epidural space: examination by cryomicrotome section. Reg Anesth Pain Med 2002; 27: 150–6.
Bhavani-Shankar K, Malov S, Hurley R, Datta S. Do rapidly administered intermittent epidural boluses provide better labor analgesia? Anesthesiology 2000; 93(Suppl): A1071.
Picard J, Crowhurst JA, Plaat F. Failure to achieve consistent anesthesia could be attributed to technique (Letter). Reg Anesth Pain Med 2001; 26: 588.
Stienstra R, Dilrosun-Alhadi BZ, Dahan A, van Kleef JW, Th Veering B, Burm AG. The epidural “top-up” in combined spinal-epidural anesthesia: the effect of volume versus dose. Anesth Analg 1999; 88: 810–4.
Leighton BL, Arkoosh VA, Huffnagle S, Huffnagle HJ, Kinsella SM, Norris MC. The dermatomal spread of epidural bupivacaine with and without prior intrathecal sufentanil. Anesth Analg 1996; 83: 526–9.
Riley ET, Ratner EF, Cohen SE. Intrathecal sufentanil for labor analgesia: do sensory changes predict better analgesia and greater hypotension? Anesth Analg 1997; 84: 346–51.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Chua, S.M.H., Sia, A.T.H. Automated intermittent epidural boluses improve analgesia induced by intrathecal fentanyl during labour. Can J Anesth 51, 581–585 (2004). https://doi.org/10.1007/BF03018402
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03018402