
Abstract
Purpose
Sevoflurane and propofol are both suitable for neuroanesthesia but have not previously been compared as maintenance agents for long duration (one to five hours) procedures.
Methods
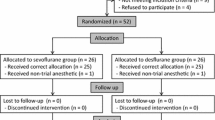
Using a multicentre international study protocol, 103 patients were randomized to receive either sevoflurane or propofol for maintenance of anesthesia during interventional neuroradiology procedures. After a standardized induction of anesthesia with propofol, 53 patients received sevoflurane 1 to 3% with 60% nitrous oxide (N2O) in oxygen (O2), and 50 patients received propofol 4 to 10 mg·kg−1·hr−1 with 60% N2O in O2. Maintenance agents were titrated against systemic arterial blood pressure (baseline mean arterial pressure ± 20%). Recovery times, changes in sedation, pain, nausea and vomiting and psychomotor function during recovery and use of rescue medication were recorded.
Results
The group receiving sevoflurane had a more rapid recovery to spontaneous ventilation, extubation, eye opening and orientation compared to the group receiving propofol (3 vs 4 min,P = 0.01; 5 vs 6min,P = 0.015; 7vs 10 min,P < 0.001; 13vs 17 min,P = 0.028; respectively). Sedation, pain, nausea and vomiting, and psychomotor function scores were similar in the two groups. Use of opioid boluses and vasopressors were similar.
Conclusion
The use of sevoflurane for maintenance of anesthesia for prolonged neuroradiological procedures is associated with more rapid early recovery than propofol and is associated with similar side effects. Sevoflurane and propofol can both be recommended for these procedures. The clinical benefit of the more rapid recovery with sevoflurane is unknown.
Résumé
Objectif
Le sévoflurane et le propofol conviennent tous les deux à la neuroanesthésie, mais n’ont jamais été comparés comme agents de maintien lors d’opérations de longue durée, soit de une à cinq heures.
Méthode
Nous avons étudié 103 patients, selon un protocole international multicentrique, qui ont reçu du sévoflurane ou du propofol pour maintenir l’anesthésie en neuroradiologie interventionnelle. À la suite d’une induction normalisée de l’anesthésie avec du propofol, 53 patients ont reçu du sévoflurane de 1 à 3 % avec 60 % de protoxyde d’azote (N2O) dans de l’oxygène (O2) et 50 patients ont reçu de 4 à 10 mg·kg− 1·h− 1 de propofol avec 60 % de N2O dans de l’O2. Les agents de maintien ont été titrés en regard de la tension artérielle générale (moyenne de la tension artérielle de base ± 20 %). Le temps nécessaire pour récupérer de l’anesthésie, les modifications de la sédation, la douleur, les nausées et les vomissements et l’état de la fonction psychomotrice pendant la récupération ainsi que l’usage de médication de secours ont été les paramètres notés.
Résultats
On a observé qu’avec le sévoflurane la reprise de la respiration spontanée, l’extubation, l’ouverture des yeux et le retour de l’orientation ont été plus précoces qu’avec le propofol (3 vs 4 min, P = 0,01 ; 5 vs 6 min, P = 0,015 ; 7 vs 10 min, P < 0,001; 13 vs 17 min, P = 0,028 ; respectivement). Les scores de sédation, de douleur, de nausées et de vomissements et de fonction psychomotrice ont été similaires chez les patients des deux groupes. L’usage de bolus d’opioïdes et de vasopresseurs a aussi été similaire.
Conclusion
L’usage du sévoflurane, comparé au propofol, pour maintenir l’anesthésie pendant les interventions neuroradiologiques prolongées, est associé à une récupération plus rapide, mais à des effets secondaires similaires. On peut donc recommander les deux médicaments pour ce type d’opérations. L’avantage clinique de la récupération précoce reliée au sévoflurane n’est pas connu.
Article PDF
Similar content being viewed by others


Avoid common mistakes on your manuscript.
References
Duffy CM, Matta BF. Sevoflurane and anesthesia for neurosurgery. A review. J Neurosurg Anesthesiol 2000; 12: 128–40.
Umbrain V, Keeris J, D’Haese J, et al. Isoflurane, desflurane and sevoflurane for carotid endarterectomy. Anaesthesia 2000; 55: 1052–7.
Smith I, White PF, Nathanson M, Gouldson R. Propofol. An update on its clinical use. Anesthesiology 1994; 81: 1005–43.
Todd MM, Warner DS, Sokoll MD, et al. A prospective, comparative trial of three anesthetics for elective supratentorial craniotomy. Anesthesiology 1993; 78: 1005–20.
Talke P, Caldwell JE, Brown R, Dodson B, Howley J, Richardson CA. A comparison of three anesthetic techniques in patients undergoing craniotomy for supratentorial intracranial surgery. Anesth Analg 2002; 95: 430–5.
Robinson BJ, Uhrich TD, Ebert TJ. A review of recovery from sevoflurane anaesthesia: comparisons with isoflurane and propofol including meta-analysis. Acta Anaesthesiol Scand 1999; 43: 185–90.
Eger EI II, Gong D, Koblin DD, et al. The effect of anesthetic duration on kinetic and recovery characteris- tics of desflurane versus sevoflurane, and on the kinetic characteristics of compound A, in volunteers. Anesth Analg 1998; 86: 414–21.
Jellish WS, Lien CA, Fontenot HJ, Hall R. The comparative effects of sevoflurane versus propofol in the induction and maintenance of anesthesia in adult patients. Anesth Analg 1996; 82: 479–85.
Watson KR, Shah MV. Clinical comparison of ‘single agent’ anaesthesia with sevoflurane versus target controlled infusion of propofol. Br J Anaesth 2000; 85: 541–6.
Ebert TJ, Robinson BJ, Uhrich TD, Mackenthun A, Pichotta PJ. Recovery from sevoflurane anesthesia. A comparison to isoflurane and propofol anesthesia. Anesthesiology 1998; 89: 1524–31.
Fredman B, Nathanson MH, Smith I, Wang J, Klein K, White PF. Sevoflurane for outpatient anesthesia: a comparison with propofol. Anesth Analg 1995; 81: 823–8.
Nathan N, Peyclit A, Lahrimi A, Feiss P. Comparison of sevoflurane and propofol for ambulatory anaesthesia in gynaecological surgery. Can J Anaesth 1998; 45: 1148–50.
Song D, Joshi GP, White PF. Titration of volatile anesthetics using bispectral index facilitates recovery after ambulatory anesthesia. Anesthesiology 1997; 87: 842–8.
Kharasch ED. Pharmacovigilance and safety aspects of sevoflurane. Acta Anaesthesiol Scand 1997; 41(Suppl 111): 146–8.
Author information
Authors and Affiliations
Corresponding author
Additional information
Support: This work was supported by Abbott Laboratories, Abbott Park, Illinois, USA.
Rights and permissions
About this article
Cite this article
Castagnini, H.E., van Eijs, F., Salevsky, F.C. et al. Sevoflurane for interventional neuroradiology procedures is associated with more rapid early recovery than propofol. Can J Anesth 51, 486–491 (2004). https://doi.org/10.1007/BF03018313
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03018313