
Abstract
Purpose
To distinguish between local and systemic drug effects, we compared pain scores, analgesic consumption and plasma concentrations after local vsiv administration of meloxicam 7.5 mg in patients with inguinal hernia repair.
Methods
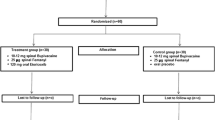
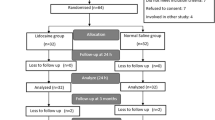
In a double-blind, randomized study 56 patients received either local oriv meloxicam 7.5 mg. Postoperative pain was assessed with a visual analogue scale (VAS) at rest, on mobilization, and on coughing, the need for supplementary analgesics (fentanyliv and/or acetaminophen-codeine tablets) was recorded, and blood samples were drawn during 24 hr after meloxicam administration.
Results
No significant differences were found between groups with respect to pain scores, or in the consumption of supplementary analgesics. Following local application of meloxicam, the peak plasma concentration (Cmax) of 0.5 ± 0.2 mg·L−1 achieved after 1.8 ± 0.5 hr was much lower than the Cmax of 2.5 ± 0.9 mg·L−1 achieved immediately afteriv administration (P < 0.05). Mean meloxicam plasma concentration after infiltration was significantly lower than afteriv doses for the first three hours after administration (P < 0.05).
Conclusion
We showed no differences in pain scores and analgesic consumption between local andiv administration of meloxicam 7.5 mg during the first 24 hr after herniorrhaphy, while plasma concentration of meloxicam was lower after local administration. These results indicate a lack of difference in pain relief after concentrating meloxicam at the hernia wound or after achieving high blood levels rapidly (iv). Local administration of meloxicam may confer an advantage over systemic administration by eliciting lower incidences of systemic adverse effects.
Résumé
Objectif
Distinguer les effets médicamenteux locaux et systémiques en comparant les scores de douleur, la consommation analgésique et les concentrations plasmatiques après l’administration locale ou iv de 7,5 mg de méloxicam chez des patients qui subissent une herniorraphie inguinale.
Méthode
II s’agit d’une étude randomisée et à double insu auprès de 56 patients qui ont reçu 7,5 mg de méloxicam local ou intraveineux. La douleur postopératoire a été évaluée avec une échelle visuelle analogique (EVA) au repos, pendant le mouvement et la toux. Le besoin d’analgésie complémentaire (fentanyl iv et/ou comprimés d’acétaminophène-codéine) a été enregistré et les échantillons sanguins prélevés pendant 24 h après l’administration de méloxicam.
Résultats
Aucune différence intergroupe significative n’a été trouvée quant aux scores de douleur ou à la consommation d’analgésique complémentaire. Après l’infiltration de méloxicam, la concentration plasmatique maximale (Cmax) de 0,5 ± 0,2 mg·L−1 atteinte après 1,8 ± 0,5 h a été plus faible que la Cmax de 2,5 ± 0,9 mg·L−1 atteinte immédiatement après l’administration iv (P < 0,05). Pendant les trois premières heures après l’administration de méloxicam, la concentration plasmatique moyenne était plus basse après l’infiltration qu’après les doses iv (P < 0,05).
Conclusion
Pendant les 24 premières heures suivant une herniorraphie, les douleurs et la consommation d’analgésique n’ont présenté aucune différence après l’administration locale ou iv de 7,5 mg de méloxicam. Mais, la concentration plasmatique de méloxicam a été plus faible après l’administration locale. La douleur nést pas mieux soulagée avec le méloxicam concentré au site de la plaie herniaire ou administré par voie iv permettant d’atteindre rapidement des concentrations plasmatiques élevées. Par ailleurs, l’infiltration pourrait réduire davantage l’incidence déffets secondaires généralisés.
Article PDF
Similar content being viewed by others

Avoid common mistakes on your manuscript.
References
Vane J. Towards a better aspirin. Nature 1994; 367: 215–6.
Meade EA, Smith WL, DeWitt DL. Differential inhibition of prostaglandin endoperoxide synthase (cyclooxygenase) isozymes by aspirin and other non-steroidal anti-inflammatory drugs. J Biol Chem 1993; 268: 6610–4.
Noble S, Balfour JA. Meloxicam. Drugs 1996; 51: 424–30.
Narjes H, Tiirck D, Busch U, Heinzel G, Nehmitz G. Pharmacokinetics and tolerability of meloxicam after i.m. administration. Br J Clin Pharmacol 1996; 41: 135–9.
Thompson JP, Sharpe P, Kiani S, Owen-Smith O. Effect of meloxicam on postoperative pain after abdominal hysterectomy. Br J Anaesth 2000; 84: 151–4.
Ferreira SH, Lorenzetti BB, Corrèa FMA. Central and peripheral antialgesic action of aspirin-like drugs. Eur J Pharmacol 1978; 53: 39–48.
Ben-David B, Katz E, Gaitini L, Goldik Z. Comparison of i.m. and local infiltration of ketorolac with and without local anaesthetic. Br J Anaesth 1995; 75: 409–12.
Mikkelsen SS, Knudsen ICE, Kristensen BB, Linnemann MUS, Frits E, Dahl JB. Comparison of tenoxicam by intramuscular injection or wound infiltration for analgesia after inguinal herniorrhaphy. Anesth Analg 1996; 83: 1239–43.
Bosek V, Cox CE. Comparison of analgesic effect of locally and sytemically administered ketorolac in mastectomy patients. Ann Surg Oncol 1996; 3: 62–6.
Ben-David B, Baune-Goldstein U, Goldik Z, Gaitini L. Is preoperative ketorolac a useful adjunct to regional anesthesia for inguinal herniorrhaphy? Acta Anaesthesiol Scand 1996; 40: 358–63.
Connelly NR, Reuben SS, Albert M, Page D. Use of preincisional ketorolac in hernia patients. Intravenous versus surgical site. Reg Anesth 1997; 22: 229–32.
Lin C-F, Wong K-L, Chan T-L, Wang J-M, Wu K-H, Wei T-T. Comparison of local infiltration of tenoxicam and intravenous tenoxicam for postoperative analgesia in herniorrhaphy. Acta Anaesthesiol Sin 1998; 36: 23–9.
Iles JDH. Relief of postoperative pain by ibuprofen: A report of two studies. Can J Surg 1980; 23: 288–90.
Dueholm S, Forrest M, Hjortsø E, Lemvigh E. Pain relief following herniotomy: a double-blind randomized comparison between naproxen and placebo. Acta Anaesthesiol Scand 1989; 33: 391–4.
Türck D, Busch U, Neinzel G, Narjes H. Clinical pharmacokinetics of meloxicam. Arzneim-Forsch 1997; 47: 253–8.
Schmid J, Busch U, Heinzel G, Bozler G, Kaschke S, Kummwr M. Meloxicam. Pharmacokinetics and metabolic pattern after intravenous infusion and oral administration to healthy subjects. Drug Metab Dispos 1995; 23: 1206–13.
Thomas DFM, Lambert WG, Lloyd Williams K. The direct perfusion of surgical wounds with local anaesthetic solution: an approach to postoperative pain? Ann R Coll Surg Engl 1983; 65: 226–9.
Yndgaard S, Holst P, Bjerre-Jepsen IC, Thomsen CB, Struckmann J, Mogensen T. Subcutaneously versus subfascially administered lidocaine in pain treatment after inguinal herniotomy. Anesth Analg 1994; 79: 324–7.
Bjune K, Stubhaug A, Dodgson MS, Breivik H. Additive analgesic effect of codeine and paracetamol can be detected in strong, but not moderate, pain after Caesarean section. Acta Anaesthesiol Scand 1996; 40: 399–407.
Collins SL, Moore RA, McQuay HJ. The visual analogue pain intensity scale: what is moderate pain in millimetres? Pain 1997; 72: 95–7.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Rømsing, J., Mysager, S., Vilmann, P. et al. Postoperative analgesia is not different after local vs systemic administration of meloxicam in patients undergoing inguinal hernia repair. Can J Anaesth 48, 978–984 (2001). https://doi.org/10.1007/BF03016587
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03016587