
Abstract
Purpose
It has been suggested that ketorolac, a non-steroidal antiinflammatory drug (NSAID) available for parenteral use, may result in prolonged (24 hr) postoperative analgesia through a peripheral mechanism when added to local anesthetic infiltration. Our objective was to assess this effect by controlling for systemic absorption of the drug.
Methods
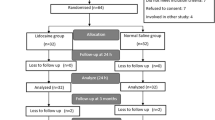
This randomized, double-blind trial studied 40 men undergoing elective inguinal hernia repair under spinal anesthesia. All patients received 19 mL of lidocaine 1% infiltrated in the operative field before incision. Patients were randomized into two groups of 20. The surgical site group received ketorolac 30 mg added to the lidocaine infiltration. In the control group, ketorolac 30 mg was injected subcutaneously in the contralateral abdominal wall. Numeric rating scores (0–10) of pain at rest and with movement were recorded at the time of discharge from the recovery room and at 24 hr postoperatively. Time to first analgesia, postoperativeiv morphine use, total time in the recovery room, and total oral analgesic use in the first 24 hr were also compared.
Results
There were no significant differences between groups with respect to any of the measured variables. In both groups, pain scores were low at rest (1.9 ± 1.4 vs 2.2 ± 1.8, surgical site and systemic groups, respectively) and moderate with movement (5.3 ± 2.2, 5.0 ± 1.8) after anesthetic recovery. Pain scores were similar at 24 hr (1.1 ± 1.3, 1.9 ± 1.6 at rest; 5.7 ± 2.0, 6.2 ± 2.2 with movement).
Conclusion
Adding ketorolac to lidocaine infiltration for hernia repair does not improve or prolong postoperative analgesia compared to systemic administration.
Résumé
Objectif
On a pensé que le kétorolac, anti-inflammatoire non stéroïdien (AINS) disponible pour usage parentéral, ajouté à une infiltration d’anesthésique local, pouvait prolonger (24 h) l’analgésie postopératoire par un mécanisme périphérique. Nous voulions évaluer cet effet en vérifiant l’absorption systémique du médicament.
Méthode
Notre étude randomisée et à double insu a porté sur 40 hommes, répartis au hasard en deux groupes de 20, devant subir une herniorraphie inguinale réglée sous rachianesthésie. Tous les patients ont reçu 19 mL de lidocaïne à 1 % par infiltration dans le champ opératoire avant l’incision. Les patients du groupe expérimental ont reçu 30 mg de kétorolac ajoutés à l’infiltration de lidocaïne. Ceux du groupe témoin ont reçu une injection sous-cutanée de 30 mg de kétorolac dans la paroi abdominale controlatérale. Les scores numériques (0–10) de douleur au repos et pendant le mouvement ont été enregistrés au départ de la salle de réveil et 24 h après l’opération. Ont aussi été comparés le temps écoulé avant la première analgésie, l’usage de morphine iv postopératoire, le temps passé à la salle de réveil et l’analgésique oral total pendant les 24 premières heures.
Résultats
Il n’y a pas eu de différences intergroupes significatives pour toutes les variables mesurées. Les scores de douleur ont été faibles au repos (1,9 ± 1,4 vs 2,2 ± 1,8, pour les groupes expérimental et témoin, respectivement) et pendant un mouvement modéré (5,3 ± 2,2, 5,0 ± 1,8) après l’anesthésie. Les scores de douleur ont été similaires à 24 h (1,1 ± 1,3, 1,9 ± 1,6 au repos; 5,7 ± 2,0, 6,2 ± 2,2 au mouvement).
Conclusion
L’ajout de kétorolac à l’infiltration de lidocaïne, comparé à l’administration systémique, n’améliore pas et ne prolonge pas l’analgésie post-herniorraphie inguinale.
Article PDF
Similar content being viewed by others


Avoid common mistakes on your manuscript.
References
Malmberg AB, Yaksh TL. Pharmacology of the spinal action of ketorolac, morphine, ST-91, U50488H and L-PIA on the formalin test and an isobolographic analysis of the NSAID interaction. Anesthesiology 1993; 79:270–81.
Lundell JC, Silverman DG, Brull SJ, et al. Reduction of postburn hyperalgesia after local injection of ketorolac in healthy volunteers. Anesthesiology 1996; 84:502–9.
Reuben SS, Connelly NR. Postoperative analgesia for outpatient arthroscopic knee surgery with intraarticular bupivacaine and ketorolac. Anesth Analg 1995; 80:1154–7.
Reuben SS, Steinberg RB, Kreitzer JM, Duprat KM. Intravenous regional anesthesia using lidocaine and ketorolac. Anesth Analg 1995; 81:110–3.
Ben-David B, Katz E, Gaitini L, Goldik Z. Comparison of i.m. and local infiltration of ketorolac with and without local anaesthetic. Br J Anaesth 1995; 75:409–12.
Connelly NR, Reuben SS, Albert M, Page D. Use of preincisional ketorolac in hernia patients: intravenous versus surgical site. Reg Anesth 1997; 22:229–32.
McGrath B, Elgendy H, Chung F, Kamming D, Curti B, King S. Thirty percent of patients have moderate to severe pain 24 hr after ambulatory surgery: a survey of 5,703 patients. Can J Anesth 2004; 51:886–91.
Reinhart DJ, Stagg KS, Walker KG, et al. Postoperative analgesia after peripheral nerve block for podiatric surgery: clinical efficacy and chemical stability of lidocaine alone versus lidocaine plus ketorolac. Reg Anesth Pain Med 2000; 25:506–13.
Ben-David B, Baune-Goldstein U, Goldik Z, Gaitini L. Is preoperative ketorolac a useful adjunct to regional anesthesia for inguinal herniorraphy? Acta Anaesthesiol Scand 1996; 40: 358–63.
Jung D, Mroszczak E, Bynum L. Pharmacokinetics of ketorolac tromethamine in humans after intravenous, intramuscular and oral administration. Eur J Clin Pharmacol 1988; 35:423–5.
Sweetman SC. Martindale. The Complete Drug Reference, 33rd ed. London: Pharmaceutical Press;2002: 49.
Kalso E. Better standardisation will improve the quality of analgesic studies. Acta Anaesthesiol Scand 1996; 40:397–8.
Gillies GW, Kenny GN, Bullingham RE, McArdle CS. The morphine sparing effect of ketorolac tromethamine. A study of a new, parenteral nonsteroidal anti-inflammatory agent after abdominal surgery. Anaesthesia 1987; 42:727–31.
Marret E, Flahault A, Samama CM, Bonnet F. Effects of postoperative, nonsteroidal, anti-inflammatory drugs on bleeding risk after tonsillectomy. Meta-analysis of randomized, controlled trials. Anesthesiology 2003; 98:1497–1502.
Author information
Authors and Affiliations
Corresponding author
Additional information
Reprints will not be available.
Rights and permissions
About this article
Cite this article
Kardash, K.J., Garzon, J., Velly, A.M. et al. Ketorolac analgesia for inguinal hernia repair is not improved by peripheral administration. Can J Anesth 52, 613–617 (2005). https://doi.org/10.1007/BF03015771
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03015771