
Abstract
Purpose: To evaluate the metabolic, hormonal and gastric fluid and pH changes after administration of a small volume of different preoperative feeding regimens.
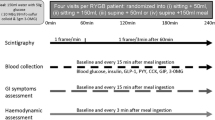
Methods: In a prospective, randomized, double-blind study 375 adult patients were allocated to one of five groups. Patients ingested 60 ml honey, glucose-fructose-sucrose-maltose mixture (GFSM), apple juice or water two hours before surgery or continued their overnight fast (controls). Blood samples were obtained from an indwelling venous catheter before the administration of feeding regimens and before induction of anesthesia for determination of glucose, triglycerides, insulin, epinephrine and norepinephrine concentrations. Before anesthesia induction, patients were asked to grade the degree of thirst and hunger. After tracheal intubation residual gastric volume (RGV) was suctioned through an orogastric tube.
Results: Administration of honey, GFSM, apple juice or water resulted in increases in RGV without changes in the gastric pH. The median RGV values were 15 ml in controls and 20–25 ml in other groups. Thirst was noted after administration of fluids containing sugars. Hunger was noted in the apple juice group. Plasma concentrations of glucose increased and triglycerides decreased after ingestion of fluids containing sugars. Plasma insulin concentrations decreased in GFSM and apple juice groups. Norepinephrine concentrations increased in the control, apple juice and water groups.
Conclusions: Small volumes of fluid increased RGV (P<0.05). Apple juice resulted in increased incidence of thirst and hunger and plasma glucose and norepinephrine concentrations. Compared with GFSM or apple juice, honey had a gentler effect on plasma glucose and insulin concentrations.
Résumé
Objectif: Évaluer les changements métaboliques et hormonaux ainsi que les modifications des liquides et du pH gastrique suivant l’administration d’un faible volume de différentes prescriptions alimentaires.
Méthode: L’étude prospective, randomisée et à double insu a été réalisée auprès de 375 patients adultes répartis au hasard en cinq groupes. Les patients ont pris 60 ml de miel, d’un mélange de glucose-fructose-sucrose-maltose (GFSM), de jus de pomme ou d’eau, deux heures avant une intervention chirurgicale, ou ils sont restés à jeun toute la nuit (témoins). Du sang a été prélevé par cathéter veineux à demeure, avant de donner les liquides et avant l’induction de l’anesthésie, pour déterminer les taux de glucose, de triglycérides, d’insuline, d’adrénaline et de noradrénaline. Les patients ont gradué leur faim et leur soif avant l’induction de l’anesthésie. Après l’intubation endotrachéale, le volume gastrique résiduel (VGR) a été aspiré dans un tube orogastrique.
Résultats: L’administration de miel, d’un mélange de GFSM, de jus de pomme ou d’eau a fait augmenter le VGR sans changer l’acidité gastrique. Le VGR moyen a été de 15 ml dans le groupe témoin et de 20–25 ml dans les autres groupes. La soif a été notée après l’administration de liquides socrés et a faim, avec l’ingestion de jus de pomme. Les concentrations plasmatiques de glucose ont augmenté et celles des triglycérides ont diminué après l’ingestion de liquides sucrés. Le taux plasmatique d’insuline a baissé avec le GFSM et le jus de pomme. Celui de la noradrénaline a diminué chez les témoins, et avec le de jus de pomme et l’eau.
Conclusion: Des volumes faibles de liquides augmentent le VGR (P <0.05). Le jus de pomme provoque une incidence accrue de faim et de soif et une augmentation des concentrations plasmatiques de glucose et de noradrénaline. Comparé au GFSM ou au jus de pomme, le miel a un effet plus modéré sur les concentrations plasmatiques de glucose et d’insuline.
Article PDF
Similar content being viewed by others


References
Mendelson CL. The aspiration of stomach contents into the lungs during obstetric anesthesia. Am J Obst Gyn 1946; 53: 191–205.
Olsson GL, Hallen B, Hambraeus-Jonzon K. Aspiration during anesthesia: a computer-aided study of 185,358 anaesthetics. Acta Anaesthesiol Scand 1986; 30: 84–92.
Rothman DL, Magnusson I, Katz LD, Shulman RG, Shulman GI. Quantitation of hepatic glycogenolysis and gluconeogenesis in fasting humans with13C NMR. Science 1991; 254: 573–6.
Marliss EB, Aoki TT, Unger RH, Soeldner JS, Cahill GF Jr. Glucagon levels and metabolic effects in fasting man. J Clin Invest 1970; 49: 2256–70.
Ljungqvist O, Boija PO, Esahili H, Larsson M, Ware J. Food deprivation alters liver glycogen metabolism and endocrine responses to hemorrhage. Am J Physiol 1990; 259: E692–8.
Maltby JR, Sutherland AD, Sale JP, Shaffer EA. Preoperative oral fluids: is a five-hour fast justified prior to elective surgery? Anesth Analg 1986; 65: 1112–6.
Sandhar BK, Goresky GV, Maltby JR, Shaffer EA. Effects of oral liquids and ranitidine on gastric fluid volume and pH in children undergoing outpatient surgery. Anesthesiology 1989; 71: 327–30.
Crawford M, Lerman J, Christensen S, Farrow-Gillespie A. Effects of duration of fasting on gastric fluid pH and volume in healthy children. Anesth Analg 1990; 71: 400–3.
Splinter WM, Schaefer JD. Ingestion of clear fluids is safe for adolescents up to 3 h before anaesthesia. Br J Anaesth 1991; 66: 48–52.
Cote CJ. NPO after mid night for children — a reappraisal (Editorial). Anesthesiology 1990; 72: 589–91.
CAS Guidelines to the practice of anesthesia. The Canadian Anaesthesiologists’ Society, 1999.
Anonymous. Practice guidelines for preoperative fasting and the use of pharmacologic agents to reduce the risk of pulmonary aspiration: application to healthy patients undergoing elective procedures. A report by the American Society of Anesthesiologist Task Force on Preoperative Fasting. Anesthesiology 1999; 90: 896’905.
Crane E. Honey. A comprehensive survey. Bee Research Association. Heinman: London, 1975.
Vardi A, Barzilay Z, Linder N, Cohen HA, Paret G, Barzilai A. Local application of honey for treatment of neonatal postoperative wound infection. Acta Paediat 1998; 87: 429–32.
Ali AT, al-Swayeh OA, al-Humayyd MS, Mustafa AA, al-Rashed RS, al-Tuwaijiri AS. Natural honey prevents ischaemia-reperfusion-induced gastric mucosal lesions and increased vascular permeability in rats. Eur J Gastroenterol Hepatol 1997; 9: 1101–7.
Cooper RA, Molan PC, Harding KG. Antibacterial activity of honey against strains of Staphylococcus aureus from infected wounds. J R Soc Med 1999; 92: 283–5.
Moore JG, Christian PE, Brown JA, et al. Influence of meal weight and caloric content on gastric emptying of meals in man. Dig Dis Sci 1984; 29: 513–9.
Maughan RJ, Leiper JB. Limitations to fluid replacement during exercise. Can J Appl Physiol 1999; 24: 173–87.
Brophy CM, Moore JG, Christian PE, Egger MJ, Taylor AT. Variability of gastric emptying measurements in man employing standardized radiolabeled meals. Dig Dis Sci 1986; 31: 799–806.
Felig P, Wahren J, Hendler R. Influence of oral glucose ingestion on splanchnic glucose and gluconeogenic substrate metabolism in man. Diabetes 1975; 24: 468–75.
Giddings AEB, Mangnall D, Rowlands BJ, Clark RG. Plasma insulin and surgery. I. Early changes due to operation in the insulin response to glucose. Ann Surg 1977; 186: 681–6.
Gerich JE, Charles MA, Grodsky GM. Regulation of pancreatic insulin and glucagon secretion. Ann Rev Physiol 1976; 38: 353–88.
Meguid MM, Aun F, Soeldner JS, Albertson DA, Boyden CM. Insulin half-life in man after trauma. Surgery 1981; 89: 650–3.
Sestoft L. An evaluation of biochemical aspects of intravenous fructose, sorbitol and xylitol administration in man. Acta Anaesthesiol Scand 1985; 82(Suppl): 19–29.
Pellaton M, Acheson K, Maeder E, Jequier E, Felber JP. The comparative oxidation of glucose, fructose, sorbitol and xylitol in normal man. J Parenter Enteral Nutr 1978; 2: 627–33.
Ionescu-Tirgoviste C, Popa E, Sintu E, Mihalache N, Cheta D, Mincu I. Blood glucose and plasma insulin responses to various carbohydrates in type 2 (non-insulin-dependent) diabetes. Diabetologia 1983; 24: 80–4.
Shambaugh P, Worthington V, Herbert JH. Differential effects of honey, sucrose, and fructose on blood sugar levels. J Manipulative Physiol Ther 1990; 13: 322–5.
Samanta A, Burden AC, Jones GR. Plasma glucose responses to glucose, sucrose, and honey in patients with diabetes mellitus: an analysis of glycaemic and peak incremental indices. Diabet Med 1985; 2: 371–3.
Ljungqvist O, Thorell A, Gutniak M, Häggmark T, Efendic S. Glucose infusion instead of preoperative fasting reduces postoperative insulin resistance. J Am Coll Surg 1994; 178: 329–36.
Author information
Authors and Affiliations
Corresponding author
Additional information
This study was carried out at King Saud University and was supported by College of Medicine Research Center.
The results of this study were presented at IARS 75th Clinical and Scientific Congress, Fort Lauderdale, Florida, MArch 16–20, 2001.
Rights and permissions
About this article
Cite this article
Naguib, M., Samarkandimb, A.H., Al-Hattab, Y. et al. Metabolic, hormonal and gastric fluid and pH changes after different preoperative feeding regimens. Can J Anesth 48, 344–350 (2001). https://doi.org/10.1007/BF03014961
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03014961