
Abstract
Purpose
To test the hypothesis that the addition of a preincisional femoral 3-in-1 block to intra-articular instillation with ropivacaine 0.2% at the end of surgery improves postoperative pain control in patients undergoing arthroscopic anterior cruciate ligament reconstruction (ACLR) under general anesthesia.
Methods
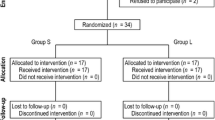
In a prospective, randomized, placebo-controlled, double-blind trial, we studied 44 patients scheduled for inpatient ACLR. Prior to incision, the treatment group (n = 22) received a femoral 3-in-1 block with 40 ml ropivacaine 0.2%, augmented by infiltrations of the lateral and anteromedial incisions with 20 ml ropivacaine 0.2% at the end of the procedure. The control group (n = 22) received saline 0.9% instead of ropivacaine. All patients received an intra-articular instillation with 30 ml ropivacaine 0.2% at the end of surgery. The primary efficacy variable was 24 hr morphine consumption postoperatively standardized by weight, administered intravenously via a patient-controlled analgesia (PCA) pump.
Results
There was no difference between both groups in 24 hr PCA morphine consumption postoperatively (control, 0.45 ± 0.44 [mean ± SD] mg·kg−1; treatment, 0.37 ± 0.50 mg·kg−1; P = 0.55). No difference was found in postoperative visual analog scale pain scores, adverse events, or vital signs. In the treatment group, R = 10/22 patients did not require postoperative morphine compared with R = 6/22 in the control group (P = 0.35).
Conclusion
We found no effect of a femoral 3-in-1 block with ropivacaine 0.2% on postoperative analgesic consumption, compared to intra-articular instillation with ropivacaine 0.2% alone, in patients undergoing ACLR under general anesthesia.
Résumé
Objectif
Vérifier l’hypothèse selon laquelle l’addition, avant l’incision, d’un blocage fémoral 3 en I à l’instillation intra- articulaire de ropivacaïne 0,2% de fin d’opération, améliore le soulagement de la douleur postopératoire chez les patients qui subissent une reconstruction arthroscopique du ligament croisé antéro-externe (RLCA) sous anesthésie générale.
Méthode
Il s’agit d’un essai prospectif randomisé en double insu contre placebo concernant 44 patients qui subissent une RLCA élective en chirurgie ambulatoire. Avant l’incision, le groupe traité (n = 22) a reçu un bloc fémoral 3 en I de 40 ml de ropivacaïne 0,2%, augmenté par des infiltrations des incisions latérale et antéromédiane de 20 ml de ropivacaine 0,2% à la fin de l’intervention. Le groupe témoin (n = 22) a reçu une solution salée à 0,9%. Tous les patients ont reçu une instillation intra-articulaire de 30 ml de ropivacaine 0,2% à la fin de l’opération. La principale variable d’efficacité a été la demande de morphine postopératoire à 24 h, uniformisée selon le poids, dont l’administration intraveineuse s’est faite à l’aide d’une pompe d’analgésie contrôlée par le patient (ACP).
Résultats
La demande postopératoire de morphine ACP à 24 h n’a pas présenté de différence intergroupe (témoin, 0,45 ± 0,44 [moyenne ± écart type]mg·kg−1; traitement, 0,37 ± 0,50 mg·kg−1; P = 0,55), ni les seuils de douleur postopératoire, selon l’échelle visuelle analogue, les effets secondaires et les signes vitaux. Dans le groupe de traitement, 10/22 patients n’ont pas demandé de morphine postopératoire et 6/22 dans le groupe témoin (P = 0,35).
Conclusion
Nous n’avons pas noté d’effet du blocage fémoral 3 en I de ropivacaïne 0,2% sur la demande postopératoire d’analgésique, comparé à l’instillation intra-articulaire de ropivacaïne 0,2% seule, chez des patients qui subissent une RLCA sous anesthésie générale.
Article PDF
Similar content being viewed by others


Avoid common mistakes on your manuscript.
References
Matheny JM, Hunks GA, Rung GW, Blanda JB, Kalenak A. A comparison of patient-controlled analgesia and continuous lumbar plexus block after anterior cruciate ligament reconstruction. Arthroscopy 1993; 9: 87–90.
Reuben SS, Steinberg RB, Cohen MA, Kilaru PA, Gibson CS. Intraarticular morphine in the multimodal analgesic management of postoperative pain after ambulatory anterior cruciate ligament repair. Anesth Analg 1998; 86: 374–8.
Marks RM, Sacher EJ. Undertreatment of medical inpatients with narcotic analgesics. Ann Int Med 1973; 78: 173–81.
Austin KL, Stapleton JV, Mather LE. Multiple intramuscular injections: a major source of variability in analgesic response to meperidine. Pain 1980; 8: 47–62.
Lynch J, Trojan S, Arhelger S, Krings-Ernst I. Intermittent femoral nerve blockade for anterior cruciate ligament repair. Use of a catheter technique in 208 patients. Acta Anaesthesiol Belg 1991; 42: 207–12.
Tetzlaff JE, Andrish J, O’Hara J Jr, Dilger J, Toon HJ. Effectiveness of bupivacaine administered via femoral nerve catheter for pain control after anterior cruciate ligament repair. J Clin Anesth 1997; 9: 542–5.
Edkin BS, Spindler KP, Flanagan JFK. Femoral nerve block as an alternative to parenteral narcotics for pain control after anterior cruciate ligament reconstruction. Arthroscopy 1995; 11: 404–9.
Winnie AF, Ramamurthy S, Durrani Z. The inguinal paravascular technic of lumbar plexus anesthesia: the “3-in-l block”. Anesth Analg 1973; 52: 989–96.
Bader AM, Datta S, Flanagan H, Covino BG. Comparison of bupivacaine-and ropivacaine-induced conduction blockade in the isolated rabbit vagus nerve. Anesth Analg 1989; 68: 724–7.
Scott DB, Lee A, Fagan D, Bowler GMR, Bloomfield P, Lundh R. Acute toxicity of ropivacaine compared with that of bupivacaine. Anesth Analg 1989; 69: 563–9.
Etches RC, Writer WDR, Ansley D, et al. Continuous epidural ropivacaine 0.2% for analgesia after lower abdominal surgery. Anesth Analg 1997; 84: 784–90.
Chirwa SS, MacLeod BA, Day B. Intraarticular bupivacaine (Marcaine) after arthrocopic meniscectomy: a randomized double-blind controlled study. Arthroscopy 1989; 5: 33–5.
Karlsson J, Rydgren B, Eriksson B, et al. Postoperative analgesic effects of intra-articular bupivacaine and morphine after arthroscopic cruciate ligament surgery. Knee Surg Sport Traumatol Arthrosc 1995; 3: 55–9.
Tierney GS, Wright RW, Smith JP, Fischer DA. Anterior cruciate ligament reconstruction as an outpatient procedure. Am J Sports Med 1995; 23: 755–6.
Brandsson S, Rydgren B, Hedner T, et al. Postoperative analgesic effects of an external cooling system and intra-articular bupivacaine/morphine after arthroscopic cruciate ligament surgery. Knee Surg Sport Traumatol Arthrosc 1996; 4: 200–5.
Denti M, Randelli P, Bigoni M, Vitale G, Marino MR, Fraschini N. Pre-and postoperative intra-articular analgesia for arthroscopic surgery of the knee and arthroscopy-assisted anterior cruciate ligament reconstruction. A double-blind randomized, prospective study. Knee Surg Sport Traumatol Arthrosc 1997; 5: 206–12.
Brown DW, Curry CM, Ruterbories LM, Avery FL, Anson PS. Evaluation of pain after arthroscopically assisted anterior cruciate ligament reconstruction. Am J Sports Med 1997; 25: 182–6.
Cepeda MS, Vargas L, Ortegon G, Sanchez MA, Carr DB. Comparative analgesic efficacy of patient-controlled analgesia with ketorolac versus morphine after elective intraabdominal operations. Anesth Analg 1995; 80: 1150–3.
Cohn BT, Draeger RI, Jackson DW. The effects of cold therapy in the postoperative management of pain in patients undergoing anterior cruciate ligament reconstruction. Am J Sports Med 1989; 17: 344–9.
Konrath GA, Lock T, Goitz HT, Scheidler J. The use of cold therapy after anterior cruciate ligament reconstruction. A prospective, randomized study and literature review. Am J Sports Med 1996; 24: 629–33.
Edwards DJ, Rimmer M, Keene GCR. The use of cold therapy in the postoperative management of patients undergoing arthroscopic anterior cruciate ligament reconstruction. Am J Sports Med 1996; 24: 193–5.
Aldrete JA, Kroulik D. A postanesthetic recovery score. Anesth Analg 1970; 49: 924–34.
Tierney E, Lewis G, Hurtig MB, Johnson D. Femoral nerve block with bupivacaine 0.25 per cent for postoperative analgesia after open knee surgery. Can J Anaesth 1987; 34: 455–8.
Fournier R, Van Gessel E, Gaggero G, Boccovi S, Forster A, Gamulin Z. Postoperative analgesia with “3-in-l” femoral nerve block after prosthetic hip surgery. Can J Anaesth 1998; 45: 34–8.
Ringrose NH, Cross MJ. Femoral nerve block in knee joint surgery. Am J Sports Med 1984; 12: 398–402.
Fanelli G, Casati A, Beccaria P, et al. A double-blind comparison of ropivacaine, bupivacaine, and mepivacaine during sciatic and femoral nerve blockade. Anesth Analg 1998; 87: 597–600.
Curry CS, Brown DL, Ruterbories L, Raessler KL. Localization of pain following arthroscopic anterior cruciate ligament repair using differential local anesthetic infiltration. (Abstract) Anesth Analg 1996; 82: S81.
Kao JT, Giangarra CE, Singer G, Martin S. A comparison of outpatient and inpatient anterior cruciate ligament reconstruction surgery. Arthroscopy 1995; 11: 151–6.
Author information
Authors and Affiliations
Corresponding author
Additional information
Supported by a grant from Astra Canada. Dr. Schwarz is recipient of a Medical Research Council of Canada (MRC) Fellowship.
Rights and permissions
About this article
Cite this article
Schwarz, S.K.W., Franciosi, L.G., Ries, C.R. et al. Addition of femoral 3-in-1 blockade to intra-articular ropivacaine 0.2% does not reduce analgesic requirements following arthroscopic knee surgery. Can J Anesth 46, 741–747 (1999). https://doi.org/10.1007/BF03013909
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03013909