
Abstract
Purpose
Pressurisation of the medullary cavity during cemented arthroplasty causes “intravasation” of marrow fat. The purpose of this study was to examine the relationship between the amount of pulmonary intravascular fat and the haemodynamic and echocardiographic changes.
Methods
Anaesthetised mongrel dogs (n = 16) underwent bilateral cemented arthroplasty (BCA) to create a large embolie load. Haemodynamic measurements included blood pressure (BP), pulmonary artery pressure (PAP), right atrial pressure and cardiac output as well as transoesophageal echocardiographic (TEE) assessment of right ventricular (RV) and left ventricular (LV) areas. Using quantitative morphometry on postmortem lung specimens, the proportion of lung tissue occluded by fat was measured.
Results
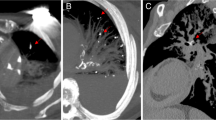
Mean BP decreased within one minute of BCA, coinciding with the appearance of echogenic material in the RV The RV area increased by 56% (P < 0.05) and LV area decreased by 34% (P < 0.05) while PAP increased from 15 ± 3 mmHg to 39 ± 10 mmHg within one minute (P < 0.001). The PAP remained elevated throughout the study (30 min). Stroke volume decreased in 14/15 dogs, yet cardiac output was maintained by increased heart rate. There was a curvilinear relationship (r=0.87) between the maximum increase in PAP and the proportion of lung occupied by fat.
Conclusion
In this model, stroke volume decreased within one minute of BCA when fat embolism accompanied prosthesis insertion. The TEE detected an increased RV area and reduced LV area associated with decreased stroke volume. The maintenance of cardiac output after intraoperative fat embolism depends primarily on the ability to increase heart rate.
Résumé
Objectif
La pressurisation de la cavité médullaire pendant rarthroplastie cimentée provoque l’«intravasation» de la graisse médullaire dans la circulation. Cette étude visait à examiner la relation entre la quantité de graisse intravasculaire interceptée au poumon et ses conséquences hémodynamiques et échocardiographiques.
Méthodes
Des chiens de race commune anesthésiés ont subi (n=16) une arthroplastie cimentée bilatérale (ACB) dans le but provoquer une forte décharge embolique. Les mesures hémodynamiques comprenaient la tension artérielle (TA), la pression artérielle pulmonaire (PAP), la mesure par l’échographie transoesophagienne (ÉTO) des surfaces du ventricule droit (VD) et du ventricule gauche (VG). La morphométrie quantitative réalisée sur des spécimens de poumons isolés a permis de mesurer la proportion du tissu pulmonaire obstrué par la graisse.
Résultats
La TA moyenne a diminué en moins d’une minute de l’ACB, ce qui coïncidait avec l’apparition de matériel échogène dans le VD. La surface du VD a augmenté de 56% (P < 0,05) et celle du VD a diminué de 34% (P < 0,05) alors que la PAP augmentait de 15 ± 3 mmHg à 39 ± 10 mmHg en moins d’une minute (P < 0,001). La PAP demeurait élevée pendant toute l’étude (30 min). Le volume d’éjection diminuait chez 14 des 15 chiens mais l’augmentation de la fréquence assurait le maintien du débit cardiaque. La relation entre l’augmentation maximale de la PAP et la proportion du poumon occupé par la graisse était curvilinéaire (r = 0,87).
Conclusion
Sur ce modèle, le volume d’éjection a diminué en moins d’une minute après l’ACB. Lembolie graisseuse suivait l’insertion de la prothèse et s’accompagnait d’une baisse du volume d’éjection. Après l’embolie graisseuse peropératoire, le maintien du débit cardiaque dépendait principalement de l’augmentation de la fréquence cardiaque.
Article PDF
Similar content being viewed by others


Avoid common mistakes on your manuscript.
References
Kallos T. Impaired arterial oxygenation associated with use of bone cement in the femoral shaft. Anesthesiology 1975; 42: 210–6.
Modig J, Busch C, Olerud S, Saldeen T, Waernbaum G. Arterial hypotension and hypoxaemia during total hip replacement: the importance of thromboplastic products, fat embolism and acrylic monomers. Acta Anaesthesiol Scand 1975; 19: 28–13.
Fitzgerald R, Mason L, Kanumilli V, Kleinhomer K, Sakamoto A, Johnson C. Transient cardiac standstill associated with embolic phenomena diagnosed by intraoperative transesophageal echocardiography during cemented total hip arthroplasty. Anesth Analg 1994; 79: 382–5.
Ereth MH, Weber JG, Abel MD, et al. Cemented versus noncemented total hip arthroplasty — embolism, hemodynamics, and intrapulmónary shunting. Mayo Clin Proc 1992; 67: 1066–74.
Christie J, Burnett R, Potts HR, Pell ACH. Echocardiography of transatrial embolism during cemented and uncemented hemiarthroplasty of the hip. J Bone Joint Surg 1994; 76-B: 409–12.
Lafont ND, Kostucki WM, Marchand PH, Michaux MN, Boogaerts JG. Embolism detected by transoesophageal echocardiography during hip arthroplasty. Can J Anaesth 1994; 41: 850–3.
Ulrich C, Burri C, Wörsdörfer O, Heinrich H. Intraoperative transesophageal two-dimensional echocardiography in total hip replacement. Arch Orthop Trauma Surg 1986; 105: 274–8.
Orsini EC, Richards RR, Mullen JM. Fatal fat embolism during cemented total knee arthroplasty: a case report. Can J Surg 1986; 29: 385–6.
Pietak S, Holmes J, Matthews RL, Petrasek A, Porter B. Cardiovascular collapse after femoral prosthesis surgery for acute hip fracture. Can J Anaesth 1997; 44: 198–201.
Byrick RJ, Mullen JB, Mazer CD, Guest CB. Transpulmonary systemic fat embolism. Studies in mongrel dogs after cemented arthroplasty. Am J Respir Crit Care Med 1994; 150: 1416–22.
Delesse MA. Procédé mécanique pour déterminer la composition des roches. C R Acad Sci (Par) 1847; 25: 544.
Barie PS, Minnear FL, Malik AB. Increased pulmonary vascular permeability after bone marrow injection in sheep. Am Rev Resp Dis 1981; 123: 648–53.
Kay JC, Noble WH, Kadiri YZ. Single versus multiple pulmonary emboli: different haemodynamic and blood gas results. Can Anaesth Soc J 1981; 28: 550–5.
Ebert PA, Allgood RJ, Jones HW III, Sabiston DC Jr. Hemodynamics during pulmonary artery occlusion. Surgery 1967; 62: 18–24.
Orsini EC, Byrick RJ, Mullen JBM, Kay JC, Waddell JP. Cardiopulmonary function and pulmonary microemboli during arthroplasty using cemented or noncemented components. The role of intramedullary pressure. J Bone Joint Surg 1987; 69-A: 822–32.
McLaughlin RE, DiFazio CA, Hakala M, et al. Blood clearance and acute pulmonary toxicity of methylmethacrylate in dogs after simulated arthroplasty and intravenous injection. J Bone Joint Surg 1973; 55-A: 1621–8.
Levine RA, Gibson TC, Aretz T, et al. Echocardiographic measurement of right ventricular volume. Circulation 1984; 69: 497–505.
Wheelwright EF, Byrick RJ, Wigglesworth DF, et al. Hypotension during cemented arthroplasty. Relationship to cardiac output and fat embolism. J Bone Joint Surg 1993; 75-B: 715–23.
Feigenbaum H. Hemodynamic information derived from echocardiography.In: Feigenbaum H (Ed.). Echocardiography. 5th ed. Philadelphia: Lea & Febiger, 1994: 207–10.
Urban MK, Sheppard R, Gordon MA, Urquhart BL. Right ventricular function during revision total hip arthroplasty. Anesth Analg 1996; 82: 1225–9.
Byrick RJ, Forbes D, Waddell JP. A monitored cardiovascular collapse during cemented total knee replacement. Anesthesiology 1986; 65: 213–6.
Guest CB, Byrick RJ, Mazer CD, Wigglesworth DF, Mullen JB, Tong JH. Choice of anaesthetic regimen influences haemodynamic response to cemented arthroplasty. Can J Anaesth 1995; 42: 928–36.
Author information
Authors and Affiliations
Corresponding author
Additional information
This study was supported by the Ontario Thoracic Society.
Rights and permissions
About this article
Cite this article
Murphy, P., Edelist, G., Byrick, R.J. et al. Relationship of fat embolism to haemodynamic and echocardiographic changes during cemented arthroplasty. Can J Anaesth 44, 1293–1300 (1997). https://doi.org/10.1007/BF03012779
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03012779