
Abstract
Purpose
Smoking affects the pharmacodynamic and pharmacokinetic behaviour of several drugs. In smokers, induction of anaesthesia is often stormy. In this study we have determined whether cigarette smoking affected thiopentone pharmacodynamic or pharmacokinetic behaviour during induction of anaesthesia.
Methods
Fifteen smokers and 15 non-smokers, scheduled for elective surgery, were studied. Heart rate, invasive arterial pressures and middle latency auditory evoked potentials were recorded awake and during thiopentone induction (9 mg·kg−1 lean body mass), before and after tracheal intubation. Blood was sampled up to 24 hr after induction to measure thiopentone plasma concentrations and to calculate pharmacokinetic parameters.
Results
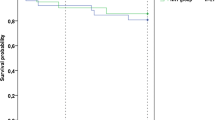
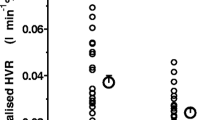
Anaesthesia was adequate in all patients, although haemodynamic intubation response was not blunted. Latencies or amplitudes of middle latency auditory evoked potentials (MLAEP) did not differ between the groups. The postintubation latencies of Nb waves were 48.9 ± 8.1 msec (mean ± SD) in smokers and 48.1 ± 8.5 msec in nonsmokers. Pharmacokinetic data showed no differences between smokers and non-smokers. Clearance of thiopentone was 2.9 ± 1.1 ml·min−1 ·kg−1 in smokers and 3.3 ± 1.0 ml·min−1 ·kg−1 in non-smokers and elimination half life of thiopentone was 12.5 ± 6.3 hr in smokers and 10.7 ± 3.1 hr in non-smokers, respectively. The haemodynamic response after the induction dose of thiopentone and after tracheal intubation were similar in smokers and non-smokers. Mean postintubation systolic arterial pressures were 192 ± 35 vs 189 ± 20 mmHg and mean postintubation heart rates were 103 ± 12 vs 102 ± 17 beat per minute (bpm) in smokers and non-smokers, respectively.
Conclusion
We conclude, that cigarette smoking does not affect the pharmacodynamic or pharmacokinetic behaviour of thiopentone.
Résumé
Objectif
Le tabagisme influence le comportement pharmacodynamique et pharmacocinétique de plusieurs produits. Chez le fumeur, l’induction de l’anesthésie est souvent mouvementée. Cette étude visait à déterminer si la cigarette affectait le comportement pharmacodynamique et phamnacocinétique du thiopental pendant l’induction de l’anesthésie.
Méthodes
Quinze fumeurs et 15 non fumeurs programmés pour une intervention non urgente participaient à l’étude. La fréquence cardiaque, la pression artérielle sanglante et les potentiels auditifs de latence moyenne ont été enregistrés à l’état vigile et pendant l’induction de l’anesthésie au thiopental (9 mg·kg−1 de poids maigre), avant et après l’intubation de la trachée. Du sang a été prélevé dans les 24 h suivant l’induction pour le dosage plasmatique du thiopental et le calcul des paramètres pharmacocinétiques.
Résultats
Tous les patients ont reçu une anesthésie satisfaisante mais sans qu’il y ait eu abolition de la réponse hémodynamique à l’intubation. Les latences ou amplitudes des potentiels évoqués auditifs de latence moyenne (MLAEP) ne différaient pas entre les groupes. Après l’intubation, la latence des ondes Nb était 48,9 ± 8,1 ms (moyenne ± ÉT) chez le fumeurs et 48,1 ± 8,5 ms chez les non fumeurs. La clairance du thiopental était de 2,9 ± 1,1 ml·min−1 ·kg−1 chez les fumeurs et de 3,3 ± 1,0 ml·min−1 ·kg−1 chez les non fumeurs; la demi-vie d’élimination du thiopental était de 12,5 ± 6,3 chez les fumeurs et de 10,7 ± 3,1 chez les non fumeurs. La réponse hémodynamique après la dose d’induction de thiopental et après l’intubation ne différait pas entre les deux groupes. Après l’intubation, la pression artérielle systolique respective des fumeurs et des non fumeurs était 192 ± 53 vs 189 ± 20 mmHg et la fréquence cardiaque moyenne respective postintubation était 103 ± 12 vs 102 ± 17 bpm.
Conclusion
La cigarette n’a pas d’influence sur le comportement phanmacodynamique et pharmacocinétique du thiopental.
Article PDF
Similar content being viewed by others

Avoid common mistakes on your manuscript.
References
Miller LG. Cigarettes and drug therapy: pharmacokinetic and pharmacodynamic considerations. Clinical Pharmacy 1990; 9: 125–35.
Miller LG. Recent developments in the study of the effects of cigarette smoking on clinical pharmacokinetics and clinical pharmacodynamics. Clin Pharmacokinet 1989; 17: 90–108.
Dawson GW, Vestal RE. Smoking and drug metabolism. Pharmacol Ther 1982; 15: 207–21.
Vähäkangas K, Pelkonen O, Sotaniemi E. Cigarette smoking and drug metabolism. Clin Pharmacol Ther 1983; 33: 375–80.
Ochs HR, Greenblatt DJ, Knüchel M. Kinetics of diazepam, midazolam, and lorazepam in cigarette smokers. Chest 1985; 87: 223–6.
Dennis A, Curran J, Sherriff J, Kinnear W. Effects of passive and active smoking on induction of anaesthesia. Br J Anaesth 1994; 73: 450–2.
Erskine RJ, Murphy PJ, Langton JA. Sensitivity of upper airway reflexes in cigarette smokers: effect of abstinence. Br J Anaesth 1994; 73: 298–302.
Dundee JW, Hassard TH, McGowan WAW, Henshaw J. The “induction” dose of thiopentone. A method of study and preliminary illustrative results. Anaesthesia 1982; 37: 1176–84.
Russo H, Brès J, Duboin M-P, Roquefeuil B. Variability of thiopental clearance in routine critical care patients. Eur J Clin Pharmacol 1995; 48: 479–87.
Hudson RJ, Stanski DR, Burch PG. Pharmacokinetics of methohexital and thiopental in surgical patients. Anesthesiology 1983; 59: 215–9.
Roizen MF. Anesthetic implications of concurrent diseases.In: Miller RD (Ed.). Anesthesia, 4th ed. New York: Churchill Livingstone Inc., 1994: 903–1014.
Schwilden H. Optimierung der dosierung volatiler anästhetika auf der grundlage pharmakokinetischdynamischer modelle. Anästhesie Intensivtherapie Notfallmedizin 1985; 20: 307–15.
Freeman DJ. Monitoring serum thiopental concentrations by liquid chromatography. Clin Chem 1981; 27: 1942–3.
Wilkinson L. SYSTAT: The System for Statistics. Evanston: SYSTAT, Inc. 1990.
Yamaoka K, Nakagawa T, Uno T. Application of Akaike’s information criterion (AIC) in the evaluation of linear pharmacokinetic equations. J Pharmacokin Biopharm 1978; 6: 165–75.
Dunne A. An iterative curve stripping technique for pharmacokinetic parameter estimation. J Pharm Pharmacol 1986; 38: 97–101.
Wagner JG. Linear Pharmacokinetic equations allowing direct calculation of many needed pharmacokinetic parameters from the coefficients and exponents of polyexponential equations which have been fitted to the data. J Pharmacokin Biopharm 1976; 4: 443–67.
Loo JCK, Riegelman S. Assessment of pharmacokintic constants from postinfusion blood curves obtained after I.V. infusion. J Pharm Sci 1970; 59: 53–5.
Thornton C. Evoked potentials in anaesthesia. Eur J Anaesthesiol 1991; 8: 89–107.
Woods DL, Clayworth CC, Knight RT, Simpson GV, Naeser MA. Generators of middleand long-latency auditory evoked potentials: implications from studies of patients with bitemporal lesions. Electroencephalogr Clin Neurophysiol 1987; 68: 132–48.
Newton DEF, Thornton C, Konieczko KM, et al. Auditory evoked response and awareness: a study in volunteers at sub-MAC concentrations of isoflurane. Br J Anaesth 1992; 69: 122–9.
Thornton C, Konieczko K, Jones JG, Jordan C, Doré CJ, Heneghan CPH. Effect of surgical stimulation on the auditory evoked response. Br J Anaesth 1988; 60: 372–8.
Schwender D, Golling W, Klasing S, Faber-Züllig E, Pöppel E, Peter K. Effects of surgical stimulation on midlatency auditory evoked potentials during general anaesthesia with propofol/fentanyl, isoflurane/fentanyl and flunitrazepam/fentanyl. Anaesthesia 1994; 49: 572–8.
Schwender D, Klasing S, Madler C, Pöppel E, Peter K. Midlatency auditory evoked potentials and purposeful movements after thiopentone bolus injection. Anaesthesia 1994; 49: 99–104.
Hung OR, Varvel JR, Shafer SL, Stanski DR. Thiopental pharmacodynamics. II. Quantitation of clinical and electroencephalographic depth of anesthesia. Anesthesiology 1992; 77: 237–44.
Kanaya N, Nakayama M, Fujita S, Namiki A. Haemodynamic and EEC changes during rapidsequence induction of anaesthesia. Can J Anaesth 1994; 41: 699–702.
Wilder-Smith OHG, Hagon O, Tassonyi E. EEG arousal during laryngoscopy and intubation: comparison of thiopentone or propofol supplemented with nitrous oxide. Br J Anaesth 1995; 75: 441–6.
Richmond CE, Matson A, Thornton C, Doré CJ, Newton DEF. Effect of neuromuscular block on depth of anaesthesia as measured by the auditory evoked response. Br J Anaesth 1996; 76: 446–8.
Flaishon R, Windsor A, Sigl J, Sebel PS. Recovery of consciousness after thiopental or propofol. Anesthesiology 1997; 86: 613–9.
Brockmöller J, Roots I. Assessment of liver metabolic function. Clinical implications. Clin Pharmacokinet 1994; 27: 216–48.
Cholerton S, Daly AK, Idle JR. The role of individual human cytochromes P450 in drug metabolism and clinical response. Trends Pharmacol Sci 1992; 13: 434–9.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Teiriä, H., Yli-Hankala, A., Neuvonen, P.J. et al. Cigarette smoking does not affect thiopentone pharmacodynamic or pharmacokinetic behaviour. Can J Anaesth 44, 1269–1274 (1997). https://doi.org/10.1007/BF03012774
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03012774