
Abstract
Purpose
To compare the accuracy of non-invasive blood pressure (NIBP) monitors in response to common cardiac arrhythmias.
Methods
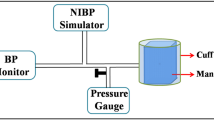
Simulated signals of normal sinus rhythm (NSR), premature ventricular contractions (PVCs), atrial fibrillation (AF) and missed beats (MB) were generated from a Cufflink™ (Dynatech Nevada) NIBP simulator. Using these signals, the Critikon 1846SX (C1846), Critikon 845xt (C845), Critikon Vital Signs (CVIT), and Hewlett Packard M1008a (HP 1008) were studied at a standard dynamic blood pressure of 120/90/80 mmHg, in order to compare monitor accuracy and signal response times.
Results
The C845 monitors most closely estimated a simulated SBP of 120 mmHg, although SBP was greater during PVCs and AF than NSR(P < 0.05). The Critikon 1846, Critikon Vital Signs, and Hewlett Packard systematically underestimated SBP during these arrhythmias, but variability was modest, as reflected by small coefficients of variation (< 2% for SBP) with all monitor types. In general, MAP and DBP were less sensitive to the effects of these arrhythmias. Finally, missed beats prolonged signal response times with all four monitor types (P < 0.05), whereas PVCs and AF did not alter this parameter.
Conclusions
This study demonstrates the extent to which the accuracy of NIBP monitors is altered by common cardiac arrhythmias. Differences in the electromechanical characteristics of these devices may help to explain the observed similarities and discrepancies.
Résumé
Objectif
Comparer la précision de différents moniteurs de tension artérielle non effractifs (TANE), lors d’arythmies cardiaques habituelles.
Méthodes
Des signaux simulés de rythme sinusal normal (RSN), d’extrasystoles ventriculaires (EV), de fibrillation auriculaire (FA) et d’arrêt sinusal (AS) ont été produits à partir d’un simulateur TANE Cufflink™ (Dynatech Nevada). En nous servant de ces signaux, nous avons étudié le Critikon 1846SX (C1846), le Critikon 845xt (C845), le Critikon Vital Signs (CVIT), et le Hewlett Packard M1008a (HP1008) selon une tension artérielle dynamique standard de 120/90/80 mmHg, dans le but de comparer la précision des moniteurs et les temps de réponse.
Résultats
Le moniteur C845 a fourni l’estimation la plus juste d’un tension artérielle systolique (TAS) simulée de 120 mmHg, bien que la TAS a été meilleure pendant l’EV et la FA que pendant le RSN (P < 0,05). Le Critikon 1846, le Critikon Vital Signs et le Hewlett Packard ont systématiquement sous-estimé la TAS pendant ces arythmies, mais la variabilité a été peu importante, comme l’indiquent les faibles coefficients de variation (< 2% pour la TAS) pour tous les types de moniteurs. En général, la tension artérielle moyenne (TAM) et la tension artérielle diastolique (TAD) ont été moins sensibles aux effets de ces arythmies. Finalement, l’arrêt sinusal a prolongé le temps de réponse avec les quatre types de moniteurs (P < 0,05), alors que les EV et la FA n’ont pas modifié ce paramètre.
Conclusion
Cette étude montre jusqu’où les arythmies cardiaques courantes modifient la précision des moniteurs de pression artérielle non effractifs. Les différentes caractéristiques électromécaniques des appareils peuvent contribuer à expliquer les similarités et les écarts observés.
Article PDF
Similar content being viewed by others

Avoid common mistakes on your manuscript.
References
Ling J, Ohara Y, Orime Y, Noon GP, Takatani S. Clinical evaluation of the oscillometric blood pressure monitor in adults and children based on the 1992 AAMI SP-10 standards. J Clin Monit 1995; 11: 123–30.
Young CC, Mark JB, White W, DeBree A, Vender JS, Fleming A. Clinical evaluation of continuous noninvasive blood pressure monitoring: accuracy and tracking capabilities. J Clin Monit 1995; 11: 245–52.
Pace NL, East TD. Simultaneous comparison of intraarterial, oscillometric, and finapres monitoring during anesthesia. Anesth Analg 1991; 73: 213–20.
White WB, Lund-Johansen P, Omvik P. Assessment of four ambulatory blood pressure monitors and measurements by clinicians versus intraarterial blood pressure at rest and during exercise. Am J Cardiol 1990; 65: 60–6.
Graettinger WF, Lipson JL, Cheung DG, Weber MA. Validation of portable noninvasive blood pressure monitoring devices: comparisons with intra-arterial and sphygmomanometer measurements. Am Heart J 1988; 116: 1155–60.
Sapinski A. Comparison of the sphygmooscillographic method with the direct and auscultatory methods of measuring blood pressure. J Clin Monit 1994; 10: 373–6.
Gorback MS, Quill TJ, Graubert DA. The accuracy of rapid oscillometric blood pressure determination. Biomed Instrum Technol 1990; 24: 371–4.
N Kim-Gau, Small CF. Review of methods and simulators for evaluation of noninvasive blood pressure monitors. Journal of Clinical Engineering 1992; 17: 469–74.
Weinger MB, Scanlon TS, Miller L. A widely unappreciated cause of failure of an automatic noninvasive blood pressure monitor. J Clin Monit 1992; 8: 291–4.
Ghosh S. Statistical Design and Analysis of Industrial Experiments. New York: Marcel Dekker Inc., 1990: 253–4.
Christensen R. Mixed models and variance components.In: Plane Answers to Complex Questions; the Theory of Linear Models. New York: Springer-Verlag Inc., 1987: 223–40.
Quill TJ. Blood pressure monitoring.In: Anesthesia Equipment: Principles and Applications: St. Louis: Mosby-Year Book Inc., 1993: 274–83.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Cleland, M.J., Pham, B. & Miller, D.R. Influence of arrhythmias on accuracy of non-invasive blood pressure monitors. Can J Anaesth 45, 699–705 (1998). https://doi.org/10.1007/BF03012103
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03012103