
Abstract
Purpose
Postoperative nausea and vomiting (PONV) is a distressing adverse effect of general anaesthesia. The aim of the current study was to compare the antiemetic activity of different 5-hydroxytryptamine3 receptor antagonists with that of metoclopramide and placebo.
Methods
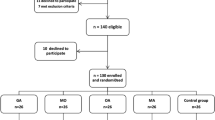
In a prospective, randomized, double-blind study we have compared the antiemetic activity of the prophylactic administration of ondansetron 4 mg, tropisetron 5 mg and granisetron 3 mg with that of metoclopramide 10 mg and placebo in 132 patients undergoing laparoscopic cholecystectomy. All study drugs and placebo were given as a short iv infusion ten minutes before the induction of anaesthesia. Perioperative anaesthetic care was standardized in all patients. Nausea and vomiting were assessed by direct questioning of the patient at 1, 4, 9, 12, 18 and 24 hr after recovery from anaesthesia. If patients experienced nausea and/or vomiting, rescue antiemetic treatment (metoclopramide 10 mg iv) was administered.
Results
For the 24-hr recovery period after surgery, the percentages of emesis-free patients were 65.5%, 52%, 48%, 29.2% and 27.6% in the ondansetron, granisetron, tropisetron, metoclopramide and placebo groups, respectively. Prophylactic antiemetic treatment with ondansetron resulted in a lower incidence (P = 0.02) of PONV than with metoclopramide or placebo. The times at which rescue antiemetic was first received were longer (P < 0.01) in ondansetron group than in the placebo and metoclopramide groups. There were no statistical differences between ondansetron, tropisetron and granisetron groups.
Conclusions
Ondansetron, when given prophylactically resulted in a significantly lower incidence of PONV than metoclopramide and placebo. Metoclopramide was ineffective.
Résumé
Objectif
Les nausées et vomissements postopératoires (NVP) sont des effets secondaires pénibles de l’anesthésie générale. L’objectif de cette étude était de comparer l’activité antiémétique de différents antagonistes des récepteurs de la 5-hydroxytryptamine avec celle de la métoclopramide et d’un placebo.
Méthode
Au cours d’une étude randomisée, prospective et en double aveugle, les auteurs ont comparé l’effet antiémétique procuré par l’administration préventive d’ondanestron 4 mg, de tropisetron 5 mg et de granisetron 3 mg avec celle de la métoclopramide 10 mg et d’un placebo chez 132 patients opérés pour une cholécystectomie par laparoscopie. Tous les médicaments à l’étude de même que le placebo ont été administrés par perfusion iv 10 min avant l’induction. La prise en charge anesthésique périopératoire a été standardisée chez tous les sujets. Les nausées et vomissements ont été évalués par l’interrogatoire personnel du patient à 1, 4, 9, 12, 18 et 24 h après le réveil. Lorsque les patients avaient des nausées et/ou des vomissements, un antiémétique de sauvetage (métoclopramide 10 mg iv) était administré.
Résultats
Pour une période de 24 h après l’intervention, le pourcentage de patients sans complication émétique a été respectivement de 65,5%, 52%, 48%, 29,2% et 27,6% pour le groupe ondansetron, granisetron, tropisetron, mêtoclopramide et placebo. L’ondansetron administré préventivement a produit une incidence plus faible (P = 0,02) de NVP que la métoclopramide et le placebo. Le délai précédant l’administration de l’antiémétique de sauvetage a été plus long (P < 0,01) dans le groupe ondansetron que dans les groupes métoclopramide et placebo. Il n’y a eu aune différence entre les groupes ondanestron, tropisetron et granisetron.
Conclusion
L’ondanestron administré préventivement a produit une incidence plus faible de NVP que la métoclopramide et le placebo. La métoclopramide n ’a pas été efficace.
Article PDF
Similar content being viewed by others


References
Editorial. Nausea and vomiting after general anaesthesia. Lancet 1989; I: 651–2.
Orkin FK. What do patients want? Preferences for immediate postoperative recovery. Anesth Analg 1992; 74: S 225.
Palazzo MGA, Strunin L. Anaesthesia and emesis. I: etiology. Can Anaesth Soc J 1984; 31: 178–87.
Way LW. Changing therapy for gallstone disease. N Engl J Med 1990; 323: 1273–4.
Taylor E, Feinstein R, White PF, Soper N. Anesthesia for laparoscopic cholecystectomy. Is nitrous oxide contraindicated? Anesthesiology 1992; 76: 541–3.
Bodner M, White PF. Antiemetic efficacy of ondansetron after outpatient laparoscopy. Anesth Analg 1991; 73: 250–4.
Zomers PJW, Langenberg CJM, De Bruijn KM. Tropisetron for postoperative nausea and vomiting in patients after gynaecological surgery. Br J Anaesth 1993; 71:677–80.
Fujii Y, Tanaka H, Toyooka H. Reduction of postoperative nausea and vomiting with granisetron. Can J Anaesth 1994; 41: 291–4.
Gold BS, Kitz DS, Lecky JH, Neuhaus JM. Unanticipated admission to the hospital following ambulatory surgery. JAMA 1989, 262: 3008–10.
Haigh CG, Kaplan LA, Durham JM, Dupeyron JP, Harmer M, Kenny GNC. Nausea and vomiting after gynaecological surgery: a meta-analysis of factors affecting their incidence. Br J Anaesth 1993; 71: 517–22.
Gan TJ, Collis R, Hetreed M. Double-blind comparison of ondansetron, droperidol and saline in the prevention of postoperative nausea and vomiting. Br J Anaesth 1994; 72: 544–7.
Larijani GE, Gratz I, Afshar M, Minassian S. Treatment of postoperative nausea and vomiting with ondansetron: a randomized, double-blind comparison with placebo. Anesth Analg 1991; 73: 246–9.
Patel RI, Hannallah RS. Anesthetic complications following pediatric ambulatory surgery: a 3-yr study. Anesthesiology 1988; 69: 1009–12.
Cohen MM, Duncan PG, DeBoer DP, Tweed WA. The postoperative interview: assessing risk factors for nausea and vomiting. Anesth Analg 1994; 78: 7–16.
Gunawardene RD, White DC. Propofol and emesis. Anaesthesia 1988; 43 (Suppl.): 65–7.
Furue H, Oota K, Taguchi T, Niitani H. Clinical evaluation of granisetron against nausea and vomiting induced by anticancer drugs (I) — optimal dose-finding study. Journal of Clinical and Therapeutic Medicine 1990; 6: 49–61.
de Bruijn KM. Tropisetron. A review of the clinical experience. Drugs 1992; 43 (Suppl. 3): 11–22.
Mikawa K, Takao Y, Nishina K, Maekawa N, Obara H. The antiemetic efficacy of prophylactic granisetron in gynecologic surgery. Anesth Analg 1995; 80: 970–4.
Wynn RL, Essien E, That PD. The effects of different antiemetic agents on morphine-induced emesis in ferrets. Eur J Pharmacol 1993; 241: 47–54.
Watcha MF, Bras PJ, Cieslak GD, Pennant JH. The doseresponse relationship of ondansetron in preventing postoperative emesis in pediatric patient undergoing ambulatory surgery. Anesthesiology 1995; 82:47–52.
Malins AF, Field JM, Nesling PM, Cooper GM. Nausea and vomiting after gynaecological laparoscopy: comparison of premedication with oral ondansetron, metoclopramide and placebo. Br J Anaesth 1994; 72: 231–3.
Desilva PHDP, Darvish AH, McDonald SM, Cronin MK, Clark K. The efficacy of prophylactic ondansetron, droperidol, perphenazine, and metoclopramide in the prevention of nausea and vomiting after major gynecologic surgery. Anesth Analg 1995; 81: 139–43.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Naguib, M., Bakry, A.K.E., Khoshim, M.H.B. et al. Prophylactic antiemetic therapy with ondansetron, tropisetron, granisetron and metoclopramide in patients undergoing laparoscopic cholecystectomy: a randomized, double-blind comparison with placebo. Can J Anaesth 43, 226–231 (1996). https://doi.org/10.1007/BF03011739
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03011739