
Abstract
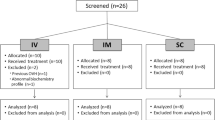
This prospective, randomized, double-blind trial evaluated the efficacy of rectal indomethacin as an adjunct to morphine for controlling postoperative pain. Fifty healthy patients undergoing elective hip arthroplasty were investigated. Group 1 (n = 25) received placebo suppositories. Group 2 (n = 25) received indomethacin suppositories, 100 mg q8hr for five doses, starting at the end of the procedure. Both groups received morphine via a PCA pump, which recorded the amount of morphine delivered each hour. After a standardized general anaesthetic, PCA was begun in the recovery room. Pain was measured with a standard 100 mm VAS at 2, 6, 20, 28, 42 hr after surgery and the morphine consumption recorded. Over the 42-hr study period, patients in Group 2 required less morphine than those in Group 1 (34.8 ± 21.8 mg vs 89.6 ± 43.7, P < 0.01). Pain scores were lower in Group 2 at 20, 28, 42 hr postoperatively. The incidence of side-effects did not differ between groups and no patient had excessive postoperative bleeding. The combination of indomethacin and morphine provided superior pain relief to morphine alone even though the control group had liberal access to morphine. This synergistic effect would make indomethacin a useful adjunct to intramuscular or epidural narcotics.
Résumé
Cette étude prospective randomisée et à double insu a évalué l’efficacité de l’indométhacine par voie rectale comme adjuvant à la morphine pour contrôler la douleur postopératoire. Cinquante patients en bonne samé devant subir une arthroplastie de la hanche élective furent investigués. Le Groupe 1 (n = 25) a reçu des suppositoires de placebo le Groupe (n = 25) a reçu des suppositoires d’indométhacine, 100 mg q8hre pour cinq doses debutant à la fin de la procédure. Les deux groupes ont reçu de la morphine à travers une pompe PCA qui a enregistre la quantité de morphine délivrée à chaque heure. Après standardisation de l’anesthésie générate, le PCA fut commencé en salle de réveil. La douleur fut mesurée avec un VAS standard 100 mm en 2, 6, 20, 28, 42 heures après la chirurgie et la consommation générate de morphine fut enregistrée. Pour une période d’étude de 42 heures, les patients du Groupe 2 ont requis moins de morphine que ceux du Groupe 1 (34.8 ± 21.8 mg vs 89.6 ± 43,7, P < 0.01). Les échelles de douleur étaient plus basses dans le Groupe 2 avant 20, 28, 42 heures après la chirurgie. L’incidence des effets secondaires n’était pas différente entre les deux groupes et aucun patient n’a demontré de saignement postoperatoire excessif. La combinaison de l’indométhacine et de la morphine a fourni un soulagement de la douleur supérieur à la morphine seule même si le groupe contrôle avait accès d’une manière libérate à la morphine. Les effets sénergétiques pourraient rendre à l’indométhacine une addition utile aux narcotiques intramusculaires ou une injection épidurale.
Article PDF
Similar content being viewed by others

Avoid common mistakes on your manuscript.
References
Spetzler B, Anderson L. Patient-controlled analgesia in the total joint arthroplasty patient. Clin Orthop 1987; 215: 122–5.
Editorial. Patient-controlled analgesia. Lancet 1980; 1: 289–90.
Maunuksela EL, Olkkola KT, Korpela R. Does prophylactic intravenous infusion of indomethacin improve the management of postoperative pain in children? Can J Anaesth 1988; 35: 123–7.
Yrjola H, Silvennoinen T, Vilppula E, Ahistrom-Bengs E. Intravenous indomethacin for postoperative pain. A double-blind study of ankle surgery. Acta Orthop Scand 1988; 59: 43–5.
Reasbeck PG, Rice ML, Reasbeck JC. Double-blind controlled trial of indomethacin as an adjunct to narcotic analgesia after major abdominal surgery. Lancet 1982; 2: 115–8.
Thind P, Sigsgaard T. The analgesic effect of indomethacin in the early postoperative period following abdominal surgery. Acta Chir Scand 1988; 154: 9–12.
Beaver W. Impact of non-narcotic oral analgesics on pain management. Am J Med1988; 84 (Suppl 5A): 3–15.
Keenan DJM, Cave K, Langdon L, Lea RE. Comparative trial of rectal indomethacin and cryoanalgesia for control of early post-thoracotomy pain. BMJ 1983; 287: 1335–7.
Boardman PL, Hart FD. Side-effects of indomethacin. Ann Rheum Dis 1967; 26: 127–32.
Keenan DJM, Cave K, Langdon L, Lea RE. Rectal indomethacin for control of postoperative pain. BMJ 1984; 288: 240.
Rane A, Oelz O, Frolich JC et al. Relation between plasma concentration of indomethacin and its effect on prostaglandin synthesis and platelet aggregation in man. Clin Pharmacol Ther 1978; 23: 658–68.
Manila MAK, Ahlstrom-Bengs E, Penttila J, Salmela J. The effect of i.v. indomethacin on bleeding time. Acta Anaesthesiol Scand 1983; 27: (Suppl 78), 72.
Taivainen T, Hitler A, Rosenberg PH, Neuvonen P. The effect of continuous intravenous indomethacin infusion on bleeding time and postoperative pain in patients undergoing emergency surgery of the lower extremities. Acta Anaesthesiol Scand 1989; 33: 58–60.
Maunuksela EL, Olkkola KT, Korpela R. Intravenous indomethacin as postoperative analgesia in children: acute effects on blood pressure, heart rate, body temperature and bleeding. Ann Clin Res 1987; 19: 359–63.
Manila MAK, Ahlstrom-Bengs E, Pekkola P. Intravenous indomethacin or oxycodone in prevention of postoperative pain. BMJ 1983; 287: 1026.
Compendium of Pharmaceuticals and Specialties 1987; 205.
Vesell ES, Passananti GT, Johnson AO. Failure of indomethacin and warfarin to interact in normal human volunteers. J Clin Pharmacol 1975; 15: 486–95.
Holt LPJ, Hawkins CF. Indomethacin: studies of absorption and of the use of indomethacin suppositories. BMJ 1965; 1: 1354–7.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Segstro, R., Morley-Forster, P.K. & Lu, G. Indomethacin as a postoperative analgesic for total hip arthroplasty. Can J Anaesth 38, 578–581 (1991). https://doi.org/10.1007/BF03008187
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF03008187