
Abstract
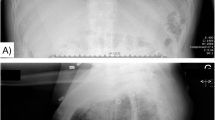
A 20 year-old female developed swelling and protrusion of the tongue and marked facial swelling while under general anaesthesia for dental restoration and gigivectomy. The initial diagnosis was angioedema; however x-rays showed marked subcutaneous emphysema more extensive in the perimandibular area with a minimal amount in the neck. There was no evidence of pneumomediastinum or pneumothorax. The iatrogenic subcutaneous emphysema was felt to be due to air-driven dental equipment. Trachéal intubation was maintained for 21 hours to prevent airway obstruction. The patient was treated with oxygen and antibiotics. Subcutaneous emphysema may occur following root canal therapy, tooth extraction, periodontal surgery and operative dentistry, due to the use of air-driven dental equipment. It has the potential to cause obstruction.
RéSUMé
Au cours d’une chirurgie dentaire avec gengivectomie, effectuée sous anesthésie générale chez une patiente de vingt ans, on a observé un œdème et une prolusion de la langue ainsi qu’un œdème marqué de la face. Le diagnostic initial a été celui d’oedème angio-neurotique. Cependant à la radiographie on a pu observer un emphysème sous-cutané important à la région péri-maxillaire et, à un degré moindre, au niveau du cou. On n’a pas trouvé de signes de pneumomédiastin ou de pneumothorax. Cet emphysème sous cutané a été considéré de cause iatrogénique, et a été attribué à l’équipement dentaire actionné à l’air comprimé. La patiente a été gardée intubée durant vingt et une heures en vue de prévenir l’obstruction des voies respiratoires, de l’oxygène lui était administré par tube en T durant cette période. Son traitement incluait également des antibiotiques. Un emphysème sous-cutané peut survenir au cours de traitements de canaux, d’extractions dentaires ou de chirurgie dentaire ou péri-dentaire lorsque le chirurgien utilise un équipement actionné à l’air comprimé.
Article PDF
Similar content being viewed by others


Avoid common mistakes on your manuscript.
References
Lloyd, R.E. Surgical emphysema as a complication in endodontics. Brit. Dent. J.138: 393 (1975).
Rhymes. R. Postextraction subcutaneous emphysema. Oral Surg.17: 271–273 (1954).
Snyder, M.B. &Rosenberg, E.S. Subcutaneous emphysema during periodontal surgery: report of acase. J. Peridontol.48: 790–791 (1977).
Hayduk, S., Bennett, R.C. &Monheim, L.M. Subcutaneous emphysema after operative dentistry: report of a case. J. Amer. Dent. Assoc.80: 1362 (1970).
Geffner, I. Subcutaneous facial emphysema following an amalgam restoration. Brit. Dent. J.148: 192 (1980).
Duncan, J.M. &Ferrillo, P.J. Interstitial emphysema after a restoration. J. Amer. Dent. Assoc.74: 407–409 (1967).
Walker, J.E.G. Emphysema of soft tissue complicating endodontic treatment using hydrogen peroxide: a case report. Brit. J. Oral Surg.13: 98 (1975).
Prupas, H.M. &Fordham, S.D. Emphysema secondary to tonsillectomy. Laryngoscope87: 1134–1136 (1977).
Brady, F.A., Roser, S.M. &Hieshima, G.B. Orbital emphysema. Brit. J. Oral Surg.14: 65–71 (1976).
Rosenberg, M.B., Wunderlich, B.K. &Reynolds, R.N. Iatrogenic subcutaneous emphysema during dental anesthesia. Anesthesiology51: 80–81 (1979).
Rickles, N.H. &Joshi, B.A. Death from air embolism during root canal therapy: a possible case in a human and an investigation in dogs. J. Amer. Dent. Assoc.67: 397–404 (1963).
Feinstone, T. Infected subcutaneous emphysema: report of acase. J. Amer. Dent. Assoc.83: 1309 (1971).
Charlebois, P.A. Three unusual cases of emphysema. Can. Anaes. Soc. J.11: 104–105 (1964).
Charlebois, P.A. Danger from the dental drill. Can. Anaes. Soc. J.11: 190–191 (1964).
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Milne, B., Katz, H., Rosales, J.K. et al. Subcutaneous facial emphysema complicating dental anaesthesia. Canad. Anaesth. Soc. J. 29, 71–73 (1982). https://doi.org/10.1007/BF03007953
Issue Date:
DOI: https://doi.org/10.1007/BF03007953