
Abstract
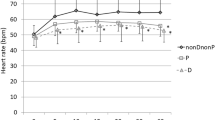
Atropine-induced heart rate (HR) changes were studied in 19 patients (ASA physical status I) during anaesthesia maintained predominantly with propofol-N2O or thiopentone-enflurane-N2O. Ten patients (Group A) received midazolam (0.07 mg · kg−1), fentanyl (1 μg · kg−1), propofol (2 mg · kg−1) and succinylcholine (1 mg · kg−1). Following tracheal intubation, anaesthesia was maintained with propofol (6 mg · kg−1 · hr−1), N2O (67 per cent) and O2 (33 per cent). In nine patients (Group B) thiopentone (4 mg · kg−1) was substituted for propofol and anaesthesia maintained with N2O (67 per cent) O2 (33 per cent), and enflurane (0.5 per cent inspired concentration). The study was non-randomised because Group B patients were only included if HR before administration of atropine < 90 beats · min−1. IPPV was performed in all patients using a Manley ventilator (minute vol. 85 ml · kg−1; tidal vol. 7 ml · kg−1). Ten minutes after tracheal intubation, incremental doses of atropine (equivalent cumulative doses: 1.8, 3.6, 7.2, 14.4, 28.8 μg · kg−1) were administered at two-minute intervals and HR responses calculated during the last 45 sec of each intervening period. No differences were observed between the groups following 1.8 and 3.6 μg · kg−1 atropine, but propofol-N2O anaesthesia was associated with reduced responses (P < 0.01) following 7.2, 14.4 and 28.8 μg · kg−1 atropine. These results suggest that there is a predominance of parasympathetic influences during propofol-N2O anaesthesia compared with thiopentone-enflurane-N2O anaesthesia.
Résumé
Les changements de la fréquence cardiaque induits par l’atropine ont éte étudiés chez 19 patients (Classe ASA I) durant l’anesthésie maintenu surtout avec du propofol-N2O ou thiopentone-enflurane-N2O. Dix patients (Groupe A) ont reçu du midazolam (0.07 mg · kg−1), fentanyl (1 μg · kg−1), propofol (2 mg · kg−1) et succinylcholine (1 mg · kg−1). Après l’intubation, l’anesthésie a été maintenue avec du propofol (6 mg · kg−1 · hr−1), N2O (67 pour cent), O2 (33 pour cent). Chez neuf patients (Groupe B) du thiopentone (4 mg · kg−1) a été substitué pour du propofol et l’anesthésie fut maintenue avec du N2O (67 pour cent), O2 (33 pour cent) et enflurane (0,5 pour cent fraction inspirée). Cette étude n’était pas randomisée car les patients du groupe B ont été inclus seulement si la fréquence cardiaque avant l’administration de l’atropine était <90 batt · min−1. La ventilation fut assurée par un ventilateur Manley chez tous les patients (vol. minute 85 ml · kg−1; volume courant 7 ml · kg−1). Dix minutes après l’intubation, des doses croissantes d’atropine (doses cumulatives: 1,8, 3,6, 7,2, 14,4, 28,8 μg · kg−1) ont été administrées à deux minutes d’intervalle et les réponses de la fréquence cardiaque furent calculées durant les dernières 45 secondes après chaque période d’intervention. Aucune différenc e fut obserée entre les groupes après 1,8 et 3,6 μg · kg−1 d’atropine mais l’anesthésie au propofol-N2O était associée avec une réponse réduite (P < 0.01) aprés 7,2, 14,4 et 28,8 μg · kg−1 d’atropine. Ces résultats suggèrent qu’il y a une prédominance de l’influence du système parasympathique lors de l’anesthésie au propofol-N2O comparativement à l’anesthésie au thiopentone-enflurane-N2O.
Article PDF
Similar content being viewed by others

Avoid common mistakes on your manuscript.
References
Claeys MA, Gepts E, Camu F. Haemodynamic changes during anaesthesia induced and maintained with propofol. Br J Anaesth 1988; 60: 3–9.
Sear JW, Shaw I, Wolf A, Kay NH. Infusions of propofol to supplement nitrous oxide-oxygen for the maintenance of anaesthesia. Anaesthesia 1988; 43 (Suppl): 18–22.
Prys-Roberts C, Davies JR, Calverley RK, Goodman NW. Haemodynamic effects of infusions of diisopropyl phenol (ICI 35868) during nitrous oxide anaesthesia in man. Br J Anaesth 1983; 55: 105–11.
Cullen PM, Turtle M, Prys-Roberts C, Way WL, Dye J. Effect of propofol anaesthesia on baroreflex activity in humans. Anesth Analg 1987; 66: 1115–20.
Hunter JM. Adverse effects of neuromuscular blocking drugs. Br J Anaesth 1987; 59: 46–60.
Adams AP. Enflurane in clinical practice. Br J Anaesth 1981; 53: 27S–41S.
Jones RM. Inhalational and intravenous anaesthetic agents.In: Anaesthesia. Nimmo WS, Smith G (Eds.). Oxford: Blackwell Scientific Publications. 1989: 34–59.
Spelina KR, Coates DP, Monk CR, Prys-Roberts C, Norley I, Turtle MJ. Dose requirements of propofol by infusion during nitrous oxide anaesthesia in man. Br J Anaesth 1986; 58: 1080–4.
Reitan JA, Stengert KB, Wymore ML, Martucci RW. Central vagal control of fentanyl induced bradycardia during halothane anaesthesia. Anesth Analg 1978; 57: 31–6.
Yamaguchi H, Dohi S, Sato S, Naito H. Heart rate response to atropine in humans anaesthetized with five different techniques. Can J Anaesth 1988; 35: 451–6.
Mirakhur RK. Anticholinergic drugs and anaesthesia. Can J Anaesth 1988; 35: 443–7.
Burks TF. The autonomic nervous system in relation to anaesthesia.In: General Anaesthesia, 5th ed. Nunn JF, Utting JE, Burnell R Brown Jr (Eds.). Oxford: Butterworths, 1989: 259–82.
Author information
Authors and Affiliations
Additional information
This study was supported in part by ICI Pharmaceuticals (UK).
Rights and permissions
About this article
Cite this article
Cross, G., Gaylard, D. & Lim, M. Atropine-induced heart rate changes: a comparison between midazolam-fentanyl-propofol-N2O and midazolam-fentanyl-thiopentone-enflurane-N2O anaesthesia. Can J Anaesth 37, 416–419 (1990). https://doi.org/10.1007/BF03005617
Issue Date:
DOI: https://doi.org/10.1007/BF03005617