
Abstract
Fundamento
Hemos analizado los resultados terapéuticos obtenidos en pacientes pediátricos diagnosticados de sarcoma de Ewing en nuestro centro y la significación de los factures de riesgo al diagnóstico sobre la supervivencia.
Pacientes y métodos
Entre los años 1980 y 1995 han sido tratados 37 pacientes. Se consideraron factores de riesgo al diagnóstico la existencia de metástasis, volumen del tumor primario mayor de 100 ml y localización centro-axial del mismo.
Resultados
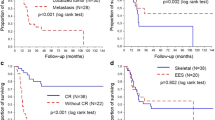
Con una mediana de seguimiento de 9 años están vivos y libres de enfermedad 25 pacientes (67,56%) y la supervivencia actuarial libre de enfermedad es del 64,86%. Los pacientes sin metástasis tuvieron una supervivencia libre de enfermedad del 74,4 frente al 16,6% de los que presentaron metástasis (p < 0,001). Los enfermos con volumen tumoral mayor de 100 ml tuvieron una supervivencia libre de enfermedad del 49,8%; no hubo ningÚn fallecimiento en el grupo de volumen tumoral menor de 100 ml. La supervivencia libre de enfermedad para los pacientes con localización periférica del tumor fue del 66,8 frente al 63% de los de localización centro-axial, diferencia que no fue estadísticamente significativa. El grupo tratado con cirugía asociada a quimioterapia obtuvo una mayor supervivencia, sin diferencias estadísticamente significativas.
Conclusiones
a) El tratamiento multidisciplinario del sarcoma de Ewing permite una curación en torno al 70% de los casos, yb) la existencia de metástasis al diagnóstico y un volumen tumoral superior a 100 ml son los dos factores de riesgo que influyen de manera significativa en la supervivencia
Abstract
Purpose
To analyze the therapeutic results obtained in pediatric patients with Ewing’s sarcoma diagnosed in our hospital and to assess the significance of risk factors at the time of diagnosis in survival.
Patients and methods
Thirty-seven patients were treated between 1980 and 1995. Metastatic disease, primary tumor volume greater than 100 ml and tumor localization in the pelvis or axis were considered to be risk factors at the time of diagnosis.
Results
Median period of observation was 9 years; 25 patients (67.56%) are alive and without evidence of disease. Estimated event-free survival (EFS) rate was 64.86%. Patients without metastatic disease had an EFS rate of 74.4%, compared with a rate of 16.6% in those with metastatic disease (p < 0.001). Patients with tumor volume greater than 100 ml had an EFS rate of 49.8%. All of the patients with tumor volume smaller than 100 ml are still alive. The EFS of patients with tumors localized in the limbs was 66.8%, compared with a rate of 63% in those with pelvis-axis localization. This difference was not statistically significant. Survival was longer in the group treated with surgery and chemotherapy, but differences were not statistically significant.
Conclusions
a) Multidisciplinary treatment of Ewing’s sarcoma yields an EFS of approximately 70%;b) metastatic disease at diagnosis and tumor volume greater than 100 ml significantly influence survival.
Similar content being viewed by others


Bibliografía
Huvos AG. Ewing’s Sarcoma. En: Huvos AG, editor. Bone tumors. Diagnosis, treatment and prognosis. Filadelfia: Saunders, 1991: 523–552.
Pritchard DJ, Dahlin DC, Dauphine RT, Taylor WF, Beabout JW. Ewing’s sarcoma. A clinicophatological and statistical analysis of patients surviving five years or longer. J Bone Joint Surg 1975; 57A: 10–16.
Falk S, Alpert M. Five year survival of patients with Ewing’s sarcoma. Surg Gynecol Osbtet 1967; 124: 319–324.
Gasparini M, Barni S, Lattuada A, Musumeci R, Bonadonna G, Fossati-Bellani F. Ten years experience with Ewing’s sarcoma. Tumori 1977; 63: 77–90.
Dahlin DC, Coventy MD, Scanion PW. Ewing’s sarcoma: a critical analysis of 165 cases. J Bone Joint Surg 1962; 43: 185–162.
Phillips RF, Higinbotham NL. Curabitity of Ewing’s endotelioma of bone in children. J. Pediatr 1987; 70: 391–397.
Nesbit ME, Pérez CA Tefft M et al. Multimodal therapy for management of primary, non-metastatic Ewing’s sarcoma. An intergroup Study. NCI Monograph 1981; 56: 255–262.
Jürgens H, Exner V, Gadner H,Göbel V, Etsfaler I. Multidisciplinary treatment of primary Ewing’s sarcoma of bone. A 6-year experience of a European Cooperative Trial. Cancer 1988; 61: 23–32.
Nesbit ME, Gehan EA, Bürgert EO et al. Multimodal therapy for the management of primary, non metastatic Ewing’s sarcoma of bone: a long-term follow-up of the first intergroup study, J Clin Oncol 1990; 8: 1664–1674.
Gasparini M, Lombardi F, Ballerini M et al. Long-term outcome of patients with monostotic Ewing’s sarcoma treated with combined modality. Med Pediatr Oncol 1994; 23: 406–412.
Craft AW, Cotterill SJ, Bullimore JA et al. Long-term results from the first UKCCSG Ewing’s Tumour Study (ET-1). Eur J Cancer 1997; 33: 1061–1069.
Göbel V, Jürgens H, Etspüler et al. Pronostic significance of tumor volume in localized Ewing’s sarcoma of bone in children and adolescents. J Cancer Res Clin Oncol 1993; 11: 1763–1769.
Evans RG, Nesbit ME, Gehan EA et al. Multimodal therapy for management of localized Ewing’s sarcoma of pelvic and sacral bones: a report from the second intergroup study. J Clin Oncol 1990; 9: 1173–1180.
Candir A, Vietty TJ, Gehan et al. Ewing’s sarcoma metastatic at diagnosis. Results and comparisons of two Intergroup Ewing’s sarcoma studies. Cancer 1990; 66: 887–893.
Ahren S, Hoffman C, Jabar S et al. Evaluation of prognostic factors in a tumor volume-adaptated treatment strategy for localized Ewing Sarcoma of bone: the CESS 86 experience. Med Pediatric Oncol 1999; 32: 186–195.
Madero L, Muñoz A, Lorenzo G, Amaya S, De Miguel C. Sarcoma de Ewing en la infancia: resultados terapéuticos. Med Clin (Bare) 1990; 95: 486–489.
Rosen G, Wollner N, Tan C, Wu SJ, Haydu SL, Chan W et al. Disease-free survival in children with Ewing’s sarcoma treated with radiation therapy and adjuvant four drug sequential chemotherapy. Cancer 1974; 33: 384–393.
Rosen G, Caparros B, Nosende C et al. Curability of Ewing’s sarcoma and considerations for future therapeutics trials. Cancer 1978; 41: 888–889.
Meyer WN, Kun L, Marina N et al. Ifosfamida plus etoposide in newly diagnosed Ewing’s sarcoma of bone. J Clin Oncol 1992; 10: 1737–1742.
Jürgens H, Cassoni A, Dunst J et al. Report from European Intergroup Cooperative Ewing’s Sarcoma study (EICESS 92). Med Pediatr Oncol 1996; 27: 264.
Sociedad Española de Oncología Pediátrica. Protocolo Nacional de Sarcoma de Ewing (SEOP 95). An Esp Pediat 1995; 45 (Supl 68): 32.
Kaplan EL, Meier P. Nonparametric estimation for incomplete observations. J Am Stat Assoc 1958; 53: 457–481.
Cox Dr. Regression models and life-tablets (with discussion). J R Statist Soc 1972; B 34: 187–220.
The Harriet Lane Handbook. Johns Hopkins Hospital. Baltimore: Mosby-year Book, Wolfe Publishing, 1991; 382.
Muñoz A, Madero L, Amaya J, Alonso MA, Miguel C. Local control and survival of Ewing’s sarcoma in children with radiotherapy and chemotherapy without radical surgery. Acta Oncol 1987; 28: 245–248.
Bacci C, Toni A, Avella M et al. Long-term results in a 144 localized Ewing’s sarcoma patients treatment with combined therapy. Cancer 1989; 63: 1477–1486.
Craft A, Cotterill A, Malcom A et al. Ifosfamide-containig chemotherapy in Ewing’s sarcoma: the second United Kingdom Children’s Cancer Study Group and Medical Research Council Ewing’s Tumor Study. J Clin Oncol 1998; 16: 3628–3633.
Paulessen M, Ahrens S, Craft AW et al. Ewing’s tumor with primary lung métastases: survival analysis of 114 (European Intergroup) cooperative Ewing’s sarcoma studies patients. J Clin Oncol 1998; 16: 3044–3052.
Madero L, Munoz A, Sanchez de Toledo J et al. Megatherapy in children with high-risk Ewing’s sarcoma in first complete remission. Bone Marrow Transplant 1998; 21: 795–799.
Ladenstein R, Lasset C, Pinkerton CR et al. Impact of megatherapy in children with high-risk Ewing’s tumours in complete remission: a report from the EBMT Solid Tumour Registry. Bone Marrow Transplant 1995; 15: 697–705.
Stewart DA, Gyonyor E, Paterson HM et al. High-dose melphalan+/- total body irradiation and autologous hematopoietic stem cell rescue for adult with Ewing’s sarcoma or peripheral neuroectodermal tumor. Bone Marrow Transplant 1996; 18: 315–318.
Blatt J, Copeland DR, Bleyer WA. Late effects of childhood cancer and its treatment. En: Pizzo PA, Pollack DG, editores. Principles and practice of pédiatrie oncology. Filadelfia: Lippicott-Raven, 1997; 1303–1330.
Craft AW. Prosthetic replacement surgery for bone tumors, cure or less cost? Br J Cancer 1991; 63: 173–175.
Robinson L. Survivors of childhood cancer and risk of a second tumour. J Nat Cancer Inst 1993; 85: 1102–1103.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Lamas, A., Maldonado, M.S., Ocete, G. et al. Sarcoma de Ewing en la infancia: resultados terapéuticos a largo plazo. Rev Oncología 2, 207–212 (2000). https://doi.org/10.1007/BF02979556
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/BF02979556