
Abstract
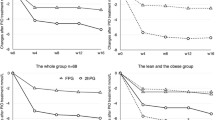
Insulin secretion dynamics and response to nateglinide were studied in patients with type 2 diabetes and reduced early-phase insulin secretion. On day 1, 24 patients underwent a 75-g oral glucose tolerance test without taking nateglinide. On day 2, they were given oral nateglinide 90 mg immediately before the oral glucose tolerance test. After glucose loading, insulin levels increased significantly at 30, 60, 90, and 120 minutes after the patients took nateglinide, along with insulinogenic indices, the total area under the insulin curve, the area under the 0- to 90-minute insulin curve, and the area under the 90- to 180-minute insulin curve. Both the plasma glucose level at 60, 90, 120, and 180 minutes and the total area under the glucose curve were significantly reduced following nateglinide administration. Compared with the low responders (n=13), the high responders (n=11) had a significantly shorter duration of disease, significantly higher insulinogenic indices in the absence of nateglinide administration, and a higher homeostasis model assessment-β cell performance. Nateglinide demonstrated a rapid-onset and rapidoffset insulin secretion-stimulating effect in this study population. A single dose of nateglinide may be indicated for patients with a relatively high homeostasis model assessment-β cell performance, a short duration of disease, and relatively high insulinogenic indices prior to nateglinide administration.
Similar content being viewed by others


References
Seltzer S, Allen EW, Herron AL Jr, Brennan MT. Insulin secretion in response to glycemic stimulus: relation of delayed initial release to carbohydrate intolerance in mild diabetes mellitus.J Clin Invest. 1967;46:323–335.
Cerasi E, Luft R, Efendic S. Decreased sensitivity of the pancreatic beta cells to glucose in prediabetic and diabetic subjects.Diabetes. 1972;21:224–234.
Ikenoue T, Okazaki K, Fujitani S, et al. Effect of a new hypoglycemic agent, A-4166 [(-)-N-(trans-4-isopropyl-cyclohexane-carbonyl)-D-phenylalanine], on postprandial blood glucose excursion: comparison with voglibose and glibenclamide.Biol Pharm Bull. 1997;20:354–359.
Ikenoue T, Akiyoshi M, Fujitani S, Okazaki K, Kondo N, Maki T. Hypoglycemic and insulinopenic effects of a novel oral antidiabetic agent, (-)-N-(trans-4-isopropylcyclohexanecarbonyl)-D-phenylalanine (A-4166).Br J Pharmacol. 1997;120:137–145.
Kosaka K, Hagura R, Kuzuya T, Kuzuya N. Insulin secretory response of diabetics during the period of improvement of glucose tolerance to normal range.Diabetologia. 1974;8:775–782.
Kadowaki T, Miyake Y, Hagura R, et al. Risk factors for worsening to diabetes in subjects with impaired glucose tolerance.Diabetologia. 1984;26:44–47.
Matthews DR, Hosker JP, Rudenski AS. Homeostasis model assessment: insulin resistance and β-cell function from fasting plasma glucose and insulin concentrations in man.Diabetologia. 1985;28:412–419.
Uchino H, Niwa M, Shimizu T, Nishikawa K, Kawamori R. Impairment of early insulin responses after glucose load, rather than insulin resistance, is responsible for postprandial hyperglycemia seen in obese type 2 diabetes: assessment using nateglinide, a new insulin secretagogue.Endocr J. 2000;14:639–641.
Uto Y, Teno S, Iwamoto Y, Omori Y, Takizawa T. Improvement of glucose tolerance by nateglinide occurs through enhancement of early phase insulin secretion.Metabolism: Clinic Exp. 2002;51:20–24.
Saloranta C, Hershon K, Ball M, et al. Efficacy and safety of nateglinide in type 2 diabetic patients with modest fasting hyperglycemia.J Clin Endocrinol Metab. 2002;87:4171–4176.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Mori, Y., Ishii, H., Hikita, M. et al. Clinical characteristics of nateglinide response as assessed by insulinogenic indices: Preliminary study to determine an optimal indication for nateglinide. Adv Therapy 20, 352–359 (2003). https://doi.org/10.1007/BF02849802
Issue Date:
DOI: https://doi.org/10.1007/BF02849802