
Abstract
Background: We have been following a cohort of patients who underwent a lumpectomy without receiving adjuvant radiotherapy or adjuvant systemic therapy. We now report the experience of a postmenopausal subgroup.
Methods: The postmenopausal subgroup included 244 patients accrued between 1977 and 1986 and followed up. The end point was ipsilateral local breast cancer recurrence. The factors studied were the patient’s age in years; tumor size (in mm); nodal status (N-, Nx, N+); estrogen and progesterone receptor status (<10, ≥10 fmol/mg protein); presence or absence of lymphovascular/perineural invasion; presence or absence, and type, of DCIS (none, non-comedo, comedo); percentage of DCIS; histological grade (1,2,3); and nuclear grade (1,2,3). Univariate analyses consisted of Kaplan-Meier plots and the Wilcoxon (Peto-Prentice) test statistic; the multivariate analyses were step-wise Cox and log-normal regressions.
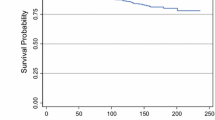
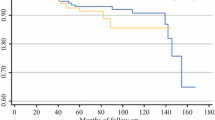
Results: The median follow-up of those patients still alive was 9.1 years, and the overall relapse rate was 24% (59/244). The univariate results indicated that the characteristics of smaller tumor size, negative nodes, positive ER status, and no lymphovascular or perineural invasion were associated with significantly (P<.05) lower relapse. From the multivariate analyses, the factors lymphovascular or perineural invasion, age, and amount of DCIS were all significantly associated with local relapse with both Cox and log-normal regressions. Additionally, there was weak evidence of an association between ER (P=.08 in the Cox regression and in the log-normal) and nodal status (P=.09 in the log-normal regression) with local relapse. We also are able to define a low-risk subgroup (N-, age ≥65, no comedo, ER positive, no emboli) with a crude 10-year local recurrence rate of 9%.
Conclusion: With longer follow-up, and for postmenopausal patients, there continues to be support for the theory that local relapse is affected by the factors lymphovascular or perineural invasion, age, amount of DCIS, ER, and nodal status. A low risk subgroup has been identified.
Similar content being viewed by others

References
McCready DR, Hanna W, Kahn HJ, et al. Factors associated with ipsilateral breast cancer recurrence after lumpectomy alone.Ann Surg Oncol 1996;3:358–66.
Chapman JW, Hanna W, Kahn HJ, et al. Alternative multivariate modelling for time to local recurrence for breast cancer patients receiving a lumpectomy alone.Surg Oncol 1996;5:265–71.
Sawka CA, Pritchard KI, Oldfield GA, et al. The Henrietta Banting Breast Centre Database: a model for clinical research utilizing a hospital-based inception cohort.J Clin Epidemiol 1995;49:779–86.
Baxter N, McCready D, Chapman J, et al. The clinical behaviour of untreated axillary nodes following local treatment for primary breast cancer.Ann Surg Oncol 1996;3:235–40.
Fisher B, Wickerham DL, Deutsch M, Anderson S, Redmond C, Fisher ER. Breast tumor recurrence following lumpectomy with and without breast irradiation: an overview of recent NSABP findings.Semin Surg Oncol 1992;8:153–60.
Hanna W, McCready DR, Chapman JW, Mobbs BG, Trudeau ME. The predictive value of ERICA in breast cancer recurrence: a univariate and multivariate analysis.Mod Pathol 1993;6:748–54.
Chapman JW, Mobbs BG, Hanna WM, et al. The standardization of estrogen receptors.J Steroid Biochem Mol Biol 1993;45:367–73.
Prentice RL, Marek P. A qualitative discrepancy between censored data rank tests.Biometrics 1979;35:861–7.
Kalbfleisch JD, Prentice RL.The Statistical Analysis of Failure Time Data. New York: John Wiley and Sons, 1980, 21–38, 179–188.
Chapman JW, Murray D, McCready DR, et al. An improved statistical approach: can it clarify the role of new prognostic factors for breast cancer?Eur J Cancer 1996;32A:1949–56.
Hanna WM, Kahn HJ, Chapman J-AW, Fish EB, Lickley HLA, McCready DR. Pathologic characteristics of breast cancer that predict for local recurrence after lumpectomy alone.Breast J 1999;5(2):105–111.
Chapman J-AW, Fish EB, Link MA. Competing risks analyses for recurrence form primary breast cancer.British J Cancer 1999;79:1508–13.
Veronesi U, Luini A, Vecchio MD, et al. Radiotherapy after breast-preserving surgery in women with localized cancer of the breast.N Engl J Med 1993;328:1587–91.
Clark RM, Whelan T, Levine M, et al. Randomized clinical trial of breast irradiation following lumpectomy and axillary dissection for node-negative breast cancer: an update.J Nat Cancer Inst 1996;88:1659–60.
Fisher B, Anderson S, Redmond CK, Wolmark N, Wickerham, Cronin WM. Reanalysis and results after 12 years of follow-up in a randomized clinical trial comparing total mastectomy with lumpectomy with or without irradiation in the treatment of breast cancer.N Engl J Med 1995;333:1456–60.
Schnitt SJ, Hayman J, Gelman R, et al. A prospective study of conservative surgery alone in the treatment of selected patients with stage I breast cancer.Cancer 1996;77:1094–1100.
Forrest AP, Stewart HJ, Everington D, et al. Randomized controlled trial of conservation therapy for breast cancer: 6-year analysis of the Scottish trial.Lancet 1996;348:708–13.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
McCready, D.R., Chapman, JA.W., Hanna, W.M. et al. Factors associated with local breast cancer recurrence after lumpectomy alone: Postmenopausal patients. Ann Surg Oncol 7, 562–567 (2000). https://doi.org/10.1007/BF02725334
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF02725334