
Abstract
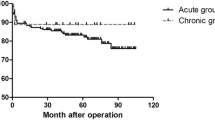
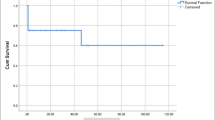
Objectives: Acute type A arch dissections are rare and no consensus has been reached on their surgical treatment. We studied perioperative risk factors for mortality in arch dissection patients.Methods: Between October 1995 and October 2001, 108 patients with acute type A dissection were operated on, of whom 16 had acute arch dissections. Their mean age was 58±9 (44–77). Surgery involved total arch replacement in 4, hemiarch replacement in 10, and intimal tear repair with pledgeted sutures and ascending aortic replacement in 2.Results: One patient who underwent total arch replacement died intraoperatively due to bleeding. Both patients who underwent ascending aortic replacement and primary repair of arch tears died 2 days postoperatively, 1 due to bleeding, and the other due to multiorgan failure. In-hospital mortality was thus 18.75%, or 3 of 16. All 3 had cardiac tamponade preoperatively. The 13 survivors were discharged after a mean hospital stay of 11±6 days. Mean follow-up was 38±25 months, from 3 months to 6 years. One patient died due to graft infection 3 months postoperatively, but the remaining 12 remain in good condition. Univariate predictors of in-hospital mortality were the type of surgery (primary intimal tear repair) (p=0.027) and preoperative cardiac tamponade (p=0.007).Conclusion: Surgical treatment of acute type A-arch dissections can be done with reasonable mortality and mid-term survival comparable with those of other subgroups with acute type A dissection. As with series of arch dissections, our patient population is too small to draw specific conclusions, but our experience leads us to conclude that the sites of intimal tears should be resected in acute type A arch dissection.
Similar content being viewed by others

References
Miller DC. Surgical management of acute aortic dissection: new data. Semin thorac Cardiovasc Surg 1991; 3: 225–37.
Roberts CS, Roberts WC. Aortic dissection with the entrance tear in transverse aorta: analysis of 12 autopsy patients. Ann Thorac Surg 1990; 50: 762–6.
Lansman SL, McCullough JN, Nguyen KH, Spielvogel D, Klein JJ, Galla JD, et al. Subtypes of acute aortic dissection. Ann Thorac Surg 1999; 67: 1975–8.
DeSanctis RW, Doroghazi RM, Austen WG, Buckley MJ. Aortic dissection. N Engl J Med 1987; 317: 1060–7.
Miller DC, Mitchell RS, Oyer PE, Stinson EB, Jamieson SW, Shumway NE. Independent determinants of operative mortality for patients with aortic dissections. Circulation 1984; 70 (Suppl I): 153–64.
Haverich A, Miller DC, Scott WC, Mitchell RS, Oyer PE, Stinson EB, et al. Acute and chronic aortic dissections: determinants of long-term outcome for operative survivors. Circulation 1985; 72 (Suppl II): 22–34.
Baumgartner FJ, Omari BO, Pandya A, Bethencourt DM. Local transverse arch repair for type A aortic dissection. Ann Thorac Surg 1997; 64: 1331–2.
Yun KL, Glower DD, Miller DC, Fann JI, Mitchell RS, White WD, et al. Aortic dissection resulting from tear of transverse arch: is concomitant arch repair warranted? J Thorac Cardiovasc Surg 1991; 102: 355–68.
Lansman SL, Raissi S, Ergin MA, Griepp RB. Urgent operation for acute transverse aortic arch dissection. J Thorac Cardiovasc Surg 1989; 97: 334–41.
Massimo CG, Presenti LF, Marranci P, Favi PP, Poma AG, Ponzalli M, et al. Extended and total aortic resection in the surgical treatment of acute type A aortic dissection: experience with 54 patients. Ann Thorac Surg 1988; 46: 420–4.
Heinemann M, Laas J, Jurmann M, Karck M, Borst HG. Surgery extended into the aortic arch in acute type A dissection. Indications, techniques, and results. Circulation 1991; 84 (Suppl III): 25–30.
Crawford ES, Kirklin JW, Naftel DC, Svensson LG, Coselli JS, Safi HJ. Surgery for acute dissection of ascending aorta. Should the arch be included? J Thorac Cardiovasc Surg 1992; 104: 469.
Kazui T, Kimura N, Yamada O, Komatsu S. Total arch graft replacement in patients with acute type A aortic dissection. Ann Thorac Surg 1994; 58: 1462–8.
Bachet J, Goudot B, Dreyfus GD, Brodaty D, Dubois C, Delentdecker P, et al. Surgery for acute type A aortic dissection: the Hopital Foch experience (1977–1998). Ann Thorac Surg 1999; 67: 2006–9.
Kazui T, Washiyama N, Muhammad B, Terada H, Yamashita K, Takinami M, et al. Extended total arch replacement for acute type A aortic dissection: experience with seventy patients. J Thorac Cardiovasc Surg 2000; 119: 558–65.
Fann JI, Smith JA, Miller DC, Mitchell RS, Moore KA, Grunkemeier G, et al. Surgical management of aortic dissection during a 30-year period. Circulation 1995; 92 (Suppl II): 113–22.
Ergin MA, Galla JD, Lansman SL, Quintana C, Bodian C, Griepp RB. Hypothermic circulatory arrest in operations on the thoracic aorta. Determinants of operative mortality and neurologicoutcome. J Thorac Cardiovasc Surg 1994; 107: 788–97.
Ergin MA, Griepp RB. Dissections of the Aorta. In: Baue AE, Geha AS, Hammond GL, Laks H, Naunheim KS, eds. Glenn's Thoracic and Cardiovascular Surgery. Vol. 2. Connecticut: Appleton & Lange, 1996: 2273–98.
Ehrlich MP, Ergin MA, McCullough JN, Lansman SL, Galla JD, Bodian CA, et al. Results of immediate surgical treatment of all acute type A dissections. Circulation 2000; 102 (Suppl III): 248–52.
David TE, Armstrong S, Ivanov J, Barnard S. Surgery for acute type A aortic dissection. Ann Thorac Surg 1999; 67: 1999–2001.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Apaydin, A.Z., Islamoglu, F., Posacioglu, H. et al. Surgical treatment of acute arch dissection. Jpn J Thorac Caridovasc Surg 51, 48–52 (2003). https://doi.org/10.1007/BF02719166
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF02719166