
Abstract
Introduction
The aim of the study was to test the combination of high-dose 4-epiadriamycin (4-epi) with cyclophosphamide in treatment-naive, stage IIIB breast cancer patients.
Material and methods
Between 1992 and 1994, 20 patients, 19 female and 1 male with locally-advanced (LA; n=9) and inflammatory (I; n=11) breast cancer were recruited. Mean age was 58 years (range 36–75 years). All patients had a Karnofsky performance status >80%. The treatment schedule was: 4-epi (120 mg/m2) and CTX (600 mg/m2) on day 1 every three weeks for three cycles. Those who achieved a complete response (CR) or a partial response (PR) underwent radical modified mastectomy, three cycles of 4-epi-cyclophosphamide (CTX), radiotherapy and tamoxifen (TMX). Patients with minor response (MR) or stable disease (SD) received hyperfractionated radiotherapy, three cycles of 4-epi-CTX and TMX.
Results
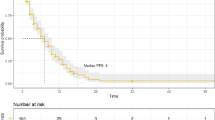
All patients were evaluable for response and survival analysis. There were 19 (95%) overall responses (OR); CR+PR:12(60%); MR:7(35%); SD:1(5%). Three of twelve (25%) patients who underwent surgery achieved a pathological complete response (PCR). In the LA group were seen 6 (66.66%) relapses and 5 (55.55%) deaths and the inflamatory group showed 5 (45.45%) relapses and 6 (54.54%) deaths. In follow-up, the median progresion free survival (PFS) of the group was 32 months (95% CI: 0–72). The patients with CR had a median of 59 months (95% CI: 12–107) compared to 20 months (95% CI: 5–35) in the patients with PR (log-rank p=0.081). Overall survival (OS) was 44 months (95% CI: 0–98), with a median of 31 months (95% CI: 24–38) for the LA patients and 44 months (95% CI: 0–93) for the I group (log-rank p=0.9822).
In general, the treatment was well tolerated, with grade 4 neutropenia in 6 (30%) patients and thrombocytopenia in 2 (10%). Nausea/vomiting grade 3–4 occurred in 4 (20%) patients and alopecia IV was 100% of patients.
Conclusions
The combination of high-dose 4-epirubicin and cyclophosphamide is safe, with a high percentage of overall response (95%), well tolerated and without cardio-toxicity.
Resumen
|Introducción
Presentamos los resultados de un estudio llevado a cabo entre 1992 y 1994, en un grupo de pacientes con cáncer de mama en estadio IIIB, tratados con 4-epiadriamicina (4-epi) a altas dosis y ciclofosfamida (CTX).
|Material y métodos
Se incluyeron 20 pacientes en estadio IIIB: localmente avanzado (LA; n=9) e inflamatorio (I; n=11); 19 mujeres y 1 hombre, con una media de edad de 58 años (rango 36–75) yperformance status Karnofsky mayor al 80%. Esquema de tratamiento: 4-epi (120 mg/m2) y CTX (600 mg/m2), día 1 cada tres semanas por tres ciclos. Las pacientes que alcanzaron respuesta completa (RC) o respuesta parcial (RP) fueron a mastectomía radical modificada, tres ciclos de 4-epi-CTX, radioterapia y tamoxifeno (TMX). Aquellas con respuesta menor (RM) o estabilización (EST) se trataron con radioterapia hiperfraccionada, tres ciclos de 4-epi-CTX y TMX.
|Resultados
Los 20 pacientes fueron valorables para análisis de respuesta y supervivencia: respuestas globales (RG):19 (95%); RC+RP:12(60%); RM:7(35%); EST:1(5%). Se intervinieron 12 pacientes con 3(25%) respuestas completas patológicas (RCP). En el grupo LA se produjeron 6 (66,66%) recidivas y 5 (55,55%) muertes y en el grupo inflamatorio 5 (45,45%) recaídas y 6 (54,54%) muertes.
La mediana de tiempo hasta la progresión (PFS) para el grupo fue de 32 meses (IC 95%: 0–72). Los pacientes con RC tuvieron una mediana de 59 meses (IC 95% 12–107) y con RP 20 meses (IC 95%: 5–35) (log-rank p=0,081). La mediana de seguimiento de la supervivencia global (SG) fue de 44 meses (IC 95%: 0–98), con una mediana de 31 meses (IC 95%: 24–38) para los LA y de 44 meses (IC 95%: 0–93) para los I (log-rank p=0,9822).
El tratamiento fue en general bien tolerado, observándose neutropenia grado 4 en 6 (30%), trombopenia en 2 (10%), emesis 3–4 en 4 (20%) y alopecia global en el 100% de los casos.
|Conclusiones
La combinación de 4-epiadriamicina a altas dosis y ciclofosfamida es segura, alcanzando un elevado porcentaje de respuestas globales (95%) con una tolerancia adecuada sin que se produjera ninguna toxicicidad cardiológica.
Similar content being viewed by others

References
Frei E. Curative cancer chemotherapy. Cancer Res 1985; 45:6523–37.
Lluch A, et al. Stage IIIB breast cancer treatment. In: EduardoDiaz-Rubio, editor. Cancer de mama. Madrid: Glaxo, 1993;p. 103–6.
Giulani FC, Coirin AK, Rice MR, Kaplan NO. Effect of 4′-doxorubicin analogues or heterotransplantation of human tumors in congenitally athimic mice. Cancer Treat Rep 1981;65:1063–75.
Fountzilas G, Inone S, Ohnuma T. Schedule-dependent interaction of cytarabine plus doxorubicin or cytarabine plus mytoxantrone in acute myelogenic leukemia cells in culture. Leukemia 1990;4:321–4.
Jain KK, Casper ES, Geler NL, et al. A prospective randomised comparison of epirubicin and doxorubicin in patients with advanced breast cancer. J Clin Oncol 1985;3:818–26.
Brambilla C, Rossi A, Bonfante V, et al. Phase II study of doxorubicin versus epirubicin in advanced breast cancer. Cancer Treat Rep 1986;70:261–6.
Hryniuk WM, Bush H. The importance of dose intensity in chemotherapy of metastatic breast cancer. J Clin Oncol 1984;2:1281–7.
Jones RB, Holland JF, Bhardwaj S, Norton L, Wilfinger C, Strashun A. A phase I–II study on intensive dose Adriamicin for advanced breast cancer. J Clin Oncol 1987;5:172–7.
Bezwoda WR, Dansey R, Seymour L. HIgh dose 4′epiadriamycin of treatment of breast cancer refractory to standard dose antracycline chemotherapy: achievement of second response. Oncology 1990;47:4–8.
Robert J. Epirubicin: clinical pharmacology and dose-effect relationship. Drugs 1990;46 (Suppl 2):20–30.
Antman K. Dose intensive therapy in breast cancer. In: Armitage JO, Antman KH, editors. High dose intensive therapy. New York: Williams & Wilkins, 1992; p. 701–18.
Hrynruk WM. Average relative dose intensity and the impact on design of clinical trials. Semin Oncol 1987;14:65–74.
Marchner N, Nagel GA, Beyer JH, Adler M, Ammon A. High-dose epirubicin in combination with cyclophosphamide (HD-EC) in advanced breast cancer: Final results of dose finding study and Phase II trial. Onkologie 1990;13:272–8.
Carmo Pereira J, Costa FO, Henriquez U, et al. A comparison of two doses of adriamycin in the primary chemotherapy of disseminated breast cancer. Br J Cancer 1987;56:471–3.
Habeshaw T, Paul J, Jones R, et al. Epirubicin at two dose levels with prednisolone as treatment for advanced breast cancer: the results of a randomised trial. J Clin Oncol 1991;9(2):295–304.
Scinto AF, Crecato MC, Boti C, et al. Phase II trial of high dose epirubicin and cyclophosphamide in advanced breast cancer. Eur J Cancer 1994;30A:1285–8.
Fountzilas G, Skarlos D, Giannakakis T, et al. Intensive chemotherapy with high dose epirubicin every 2 weeks and prophylactic administration of Filgrastim in advanced breast cancer. Eur J Cancer 1994;30A:965–9.
Cognetti F, Scinto AF, Cercato MC, et al. Phase II trial of high dose epirubicin (HD-EPI) and cyclophosphamide (CTX) every two weeks+R-met-hug-CSF in locally advanced and metastatic breast cancer. Proc Annu Meet Am Soc Clin Oncol 1994;13:A155.
Levi JA, Beith JM, Snider RD, Tattersall MH, Bell D, Wheeler H. Phase II study of high dose epirubicin in combination with cyclophosphamide in patients with advanced breast cancer. Aust N Z J Med 1995;25(5): 474–8.
Bordenave RH, Pelati M, Cuevas A, Paz G. Tratamiento del cáncer de mama avanzado con epirrubicina a altas dosis y ciclofosfamida. Neoplasia 1966; 13:7–11.
Hortobagyi GN, Bodney GP, Buzdar AU, et al. Evaluation of high dose versus standard FAC chemotherapy for advanced breast cancer in protected environment units: A prospective randomize study. J Clin Oncol 1987;5:354–64.
Ebbs SR, Saunders JA, Graham H, A'Hern RP, Bates T, Baum M. Advanced breast cancer. A randomised trial of epirubicin at two different dosages and two administration systems. Acta Oncol 1989;28:887–92.
Focan C, Andrien JM, Closon MT, et al. Dose-response relationship of epirubicin-based first-line chemotherapy for breast cancer. The results of a randomised trial. J Clin Oncol 1993;11:1253–63.
Bonnefoi H, Diebold-Berger S, Therasse P, et al. Locally advanced/inflammatory breast cancers treated with intensive epirubicin-based neoadyuvant chemotherapy: are there molecular markers in the primary tumour that predict for 5-year clinical outcome? Ann Oncol 2003;14:406–13.
Perez DJ, Harvey VJ, Robinson BA, et al. A randomised comparison of single-agent doxorubycin and epirubicin as first line cytotoxic therapy in advanced breast cancer. J Clin Oncol 1991;9:2148–52.
Limat S, Demesmay K, Voillat L, et al. Early cardiotoxicity of the CHOP regimen in aggressive non Hodgkin's lymphoma. Ann Oncol 2003;14:277–81.
Swain S, Whaley F, Ewer M. Congestive heart failure in patients treated with doxorubicin. A retrospective analysis of three trials. Cancer 2003;97(11):2869–79.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Sarmiento, U.B., Morales, J.A., Bujanda, D.A. et al. High dose epirubicin and cyclophosphamide in breast cancer stage IIIB. Rev Oncol 6, 347–352 (2004). https://doi.org/10.1007/BF02710064
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/BF02710064