
Abstract
In our institution, the selection of patients who require thoracic aortography to evaluate for acute traumatic aortic injury (ATAI) is based upon an appropriate mechanism of injury and radiologic demonstration of a mediastinal hematoma. When plain chest or chest and/or mediastinal radiographs demonstrate a mediastinal hematoma, the patient undergoes thoracic aortography as promptly as is clinically feasible. If the plain film studies are negative for mediastinal hematoma, thoracic aortography is not performed because the patient is presumed not to have an ATAI.
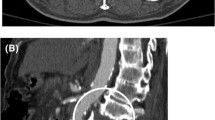
When the plain film studies are equivocal and the patient is stable, unenhanced computed tomography (CT) of the mediastinum is used to evaluate for a mediastinal hematoma. CT signs of a mediastinal hematoma include a soft tissue density, representing the hematoma admixed with mediastinal fat, which obscures or obliterates the normal aortic-mediastinal fat interface; hematoma admixed with fat of the right paratracheal stripe causing increased width and density of the stripe; and hematoma surrounding, and frequently displacing, the esophagus to the right of its normal position.
Six of 36 patients (17%) with mediastinal hematoma demonstrated by unenhanced mediastinal CT had ATAI by thoracic aortography and confirmed surgically. The thoracic aortograms of the remaining 30 of 36 patients (83%) were negative.
Sixty-three of 100 patients (63%) with equivocal plain chest or mediastinal radiographs had negative mediastinum by unenhanced CT. All 63 patients (100%) with normal mediastinal CT and who did not have thoracic aortography were discharged from the hospital 1–42 days (mean, 9.3 days) post-injury without clinical or radiographic signs of aortic rupture.
Similar content being viewed by others


References
Mirvis SE, Kostrubiak I, Whitley NO, Goldstein LD, Rodriguez A. Role of CT in excluding major arterial injury after blunt thoracic trauma. AJR Am J Roentgenol 1987;149:601–5.
Madayag MA, Kirshenbaum KJ, Nadimpalli SR, et al. horacic aortic trauma: role of dynamic CT. Radiology 1991;179:853–5.
Morgan PW, Goodman LR, Aprahamian C, et al. Evaluation of traumatic aortic injury: does dynamic contrast-enhanced CT play a role? Radiology 1992;182:661–6.
Raptopoulos V, Sheiman RG, Phillips DA, et al. Traumatic aortic tear: screening with chest CT. Radiology 1992;182:667–73.
Richardson P, Mirvis SE, Scorpio R, Dunham CM. Value of CT in determining the need for angiography when findings of mediastinal hemorrhage on chest radiographs are equivocal. AJR Am J Roentgenol 1991;156:273–9.
Brooks AP, Olson LK, Shakford SR. Computed tomography in the diagnosis of traumatic rupture of the aorta. Clin Radiol 1989;40:133–8.
Ishikawa T, Nakajima Y, Kaji T. The role of CT in traumatic rupture of the thoracic aorta and its proximal branches. Semin Roentgenol 1989;24:38–46.
Heiberg E, Wolverson MK, Sundaram M, Shields JB. CT in aortic trauma. AJR Am J Roentgenol 1983;140:1119–24.
Kerns SC, Gay SB. CT of blunt chest trauma. AJR Am J Roentgenol 1990;154:55–60.
Kubota RT, Trip MD, Tisnado J, Cho SR. Evaluation of traumatic rupture of descending aortic by aortography and computer tomography: case report with follow-up. J Comput Assist Tomogr 1985;9:237–40.
White RD, Lipton MJ, Higgins CB, et al. Non-invasive evaluation of suspected thoracic aortic disease by contrast-enhanced computed tomography. Am J Cardiol 1986;57:287–90.
Parmley LF, Mattingly TW, Manion WC, et al. Nonpenetrating traumatic injury of the aorta. Circulation 1958;17:1086–101.
Heitzman ER. The mediastinum: radiological correlations with anatomy and pathology. 2nd ed. Berlin: Springer-Verlag, 1988;187.
Sevitt S. Traumatic ruptures of the aorta: a clinico-pathologic study. Injury 1977;8:159–73.
Lundveall J. The mechanism of traumatic rupture of the aorta. Acta Pathol Microbiol Scand 1964;62:34–46.
Soyer R, Burnett A, Piwanica A, et al. Traumatic rupture of the aorta with reference to 34 operated cases. J Cardiovasc Surg 1981;22:103–8.
Boball AJ Jr, Arbagast NR, Ripepi AC, et al, Aortic laceration due to rapid deceleration. Arch Surg 1969;98:595–601.
Turney SZ, Attar S, Ayella R. Traumatic rupture of the aorta. J Thorac Cardiovasc Surg 1976;72:727–34.
Baron RL, Lee JKT, Sagal SS, Peterson RT. Computed tomography of the normal thymus. Radiology 1982;142:121–5.
Hines M, Harris JH Jr. CT characteristics of the normal thymus gland: relationship to mediastinal hematoma. Emerg Radiol 1995 (in press).
Author information
Authors and Affiliations
Additional information
Supported in part by the John S. Dunn Research Foundation.
Rights and permissions
About this article
Cite this article
Harris, J.H., Horowitz, D.R. & Zelitt, D.L. Unenhanced dynamic mediastinal computed tomography in the selection of patients requiring thoracic aortography for the detection of acute traumatic aortic injury. Emergency Radiology 2, 67–76 (1995). https://doi.org/10.1007/BF02628782
Issue Date:
DOI: https://doi.org/10.1007/BF02628782