
Abstract
Background: While inverted nipples are a common problem, mammary fistulas are very rare. A mammary duct ectasia is both consequence of and reason for a nipple retraction.
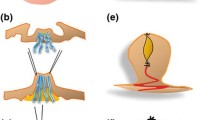
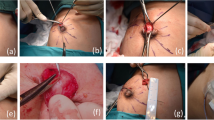
Methods: In the following an operative technique is introduced which includes pathophysiological and cosmetical aspects. From a periareolar incision the ducti lactiferi can be isolated and transsected. Thus, the nipple can easily be everted and kept in this position via transfixation.
Results: In 20 out of 28 cases this technique led to excellent cosmetic results. Within a follow up period of 2 years recurrence was observed in 2 cases.
Conclusions: Due to the unspecifity of the accompanying symptoms, operative treatment should easily be indicated. Inflammation and purulent secretion can also be caused by cancer, in case of long — lasting existence they lead to aesthetic deformation.
Zusammenfassung
Grundlagen: Während Hohlwarzen häufig sind, ist die Mammafistel sehr selten. Das Auftreten einer Milchgangsektasie ist sowohl Folge als auch Ursache einer Hohlwarze.
Methodik: Hier wird eine Operationstechnik vorgestellt, die sowohl pathophysiologischen als auch kosmetischen Aspekten Rechnung trägt. Von einer periareolaren Inzision aus werden die Milchgänge dargestellt und durchtrennt. Anschließend läßt sich der Nippel leicht evertieren und kann durch Transfixation in Position gehalten werden.
Ergebnisse: Bei 20 von 28 Patienten konnte ein ausgezeichnetes kosmetisches Ergebnis mit dieser Technik erreicht werden. Innerhalb einer Nachbeobachtungszeit von 2 Jahren trat bei 2 Patientinnen ein Rezidiv auf.
Schlußfolgerungen: Die Indikation zur operativen Korrektur sollte frühzeitig gestellt werden, da die begleitenden Symptome unspezifisch sind: Entzündung und eitrige Sekretion können auch durch ein Mammakarzinom verursacht sein, bei längerem Bestehen nimmt die ästhetische Deformierung zu.
Similar content being viewed by others

References
Abramson OJ: Mammary duct ectasia, mamillary fistula and subareolar sinuses. Arch Surg 1969;169:217–226.
Aitken RJ, Hood J, Going JJ, Miles RS, Forrest APM: Bacteriology of mammary duct ectasia. Br J Surg 1988;75:1040–1041.
Bundred NJ, Dixon, JM, Lumsden AB, Radford D, Hood J, Miles RS, Ghetty U, Forrest APM: Are the lesions of duct ectasia sterile? Br J Surg 1985;72:844–845.
Bundred NJ, Dixon JM, Chetty LL, Forrest APM: Mamillary fistula. Br J Surg 1987;74:466–468.
Devitt JE: Management of nipple discharge by clinical findings. Am J Surg 1985;149:789–792.
Dixon JM, Thompson AM: Effective surgical treatment for mammary duct fistula. Br J Surg 1991;78:1185–1186.
Hartley MN, Stewart J, Benson EA: Subareolar dissection for duct ectasia and periareolar sepsis. Br J Surg 1991;78:1187–1188.
Jaeger K, Giebel GD, Kockskämper C, Horch R: Mamma fistulans-Ergebnisse der chirurgischen Therapie. Chir Praxis 1989;41:737–742.
Lambert ME, Betts CD, Sollwood RA: Mamillary fistula. Br J Surg 1986;73:367–368.
Lemperle G, Nievergelt J: Plastische Mammachirurgie-Ein Operationsatlas. Berlin, Springer, 1989.
Maier WP, Berger A, Derrick BM: Periarcolar abscess in the nonlactating breast. Am J Surg 1982;144:359–361.
Pearson HE: Bacteroides in areolar breast abscesses. Surg Gynecol Obstet 1967;125:800–802.
Sandison AT, Walker JC: Inflammatory mastitis, mammary duct ectasia and mamillary fistulas. Br J Surg 1962;50:57–64.
Thomas WG, Williamson RCN, Davies JD, Webb AJ: The clinical syndrome of mammary duct ectasia. Br J Surg 1982;69:423–425.
Welch M, Durrans D, Gonzalez J, Daya H, Owen AMWC: Microdochectomy for discharge from a single lactiferous duct. Br J Surg 1990;77:1213–1214.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Giebel, G.D., Jaeger, K. & Stark, G.B. Duct transsection and transfixation — Eversion of the nipple as causative treatment for mamillary fistula. Acta Chir Austriaca 26, 417–418 (1994). https://doi.org/10.1007/BF02620050
Issue Date:
DOI: https://doi.org/10.1007/BF02620050