
Summary
Background: Lung Volume Reduction Surgery (LVRS) is a new surgical approach in patients with severe, non-bullous lung emphysema. Although it was first described byBrantigan in 1957,Cooper reintroduced the technique 1995 into surgical practice. Selection of patients for LVRS is based on history, clinical investigation, chest X-ray, lung function testing with blood gas analysis, measurement of ventilatory mechanics and CT-scan. Selection criteria are severe emphysema (FeV1<35 % predicted, RV>250 % predicted, TLC>130 % predicted), dyspnea despite optimized medical therapy, radiological signs of hyperinflation, heterogeneity of disease and impaired ventilatory mechanics. Once a patient is accepted for the procedure he should enter a rehabilitation program to optimize his overall condition and exercise endurance. Selection of patients for LVRS is based on history, clinical investigation, chest X-ray, lung function testing with blood gas analysis, measurement of ventilatory mechanics and CT-scan. Selection criteria are severe emphysema (FeV1<35 % predicted, RV \s>250% predicted, TLC\s>130 % predicted), dyspnea despite optimized medical therapy, radiological signs of hyperinflation, heterogeneity of disease and impaired ventilatory mechanics. Once a patient is accepted for the procedure he should enter a rehabilitation program to optimize his overall condition and exercise endurance.
Methods: Excision of peripheral lung segments is performed with stapling devices. Usually it is achieved to resect about 30 % of lung tissue. With removal of the most diseased parts of the lung, LVRS intends to reduce residual and total lung volume, to bring the diaphragm back to a normal position and to restore transdiaphragmatic pressure generation. Recent studies have demonstrated improvements in pulmonary function. ventilatory mechanics, exercise tolerance and quality of life in selected patients following LVRS. However some questions regarding overall benefit, optimal patient selection, operative techniques and duration of response still remain undefined.
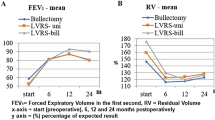
Results: In our own experience, between September 1994 and May 1998 LVRS was performed through median sternotomy (n=15), videoendoscopically (n=49), by thoracotomy (n=18) or combined, videoendoscopically on one side, thoracotomy on the other (n=9) in 91 patients (age 33–80 years; mean 56.4 years). Perioperative mortality was 5.5 % (5 patients). Mean FeV1 significantly increased by 28.6 % from 25.5±1.2 % preoperatively to 32.8±1.9 % after the first 6 months postoperatively (p<0.05). Mean RV was reduced from 320.3±7.9 %, preoperatively to 248.4±7.5 % 6 months post-operatively and mean TLC from 140.2±2.4 % to 126.1±2.11 % (p<0.05). Intrinsic PEEP decreased significantly from 5.1±0.4 cm H2O preoperatively to 2.3±0.3 cm H2O postoperatively (p<0.05).
Conclusions: These results suggest LVRS as an excellent therapeutic option for selected patients with severe emphysema and additional signs of severe hyperinflation. LVRS offers the possibility of significant postoperative functional improvement and marked increase in quality of life.
Zusammenfassung
Grundlagen: Die Lungenvolumenreduktion (LVRS) ist ein neues chirurgisches Verfahren bei Patienten mit schwerem, nichtbullösem Lungenemphysem. Obwohl LVRS erstmals 1957 vonBrantigan beschrieben wurde, führteCooper 1995 die Technik wieder in die chirurgische Praxis ein. Die Patientenselektion für LVRS basiert auf Anamnese, klinischer Untersuchung, Thoraxröntgen, Lungenfunktion mit Blutgasanalyse. Vermessung der Atemmechanik und CT-Untersuchung. Die Selektionskriterien sind schweres Emphysem (FeV1<35 % des Sollwertes, RV > 250 % des Sollwertes. TLC > 130 % des Sollwertes), Dyspnoe trotz optimaler medikamentöser Therapie, radiologische Zeichen der Überblähung sowie Heterogenität der Erkrankung und eingeschränkte Atemmechanik. Wird ein Patient für das Verfahren ausgewählt, soll er ein Rehabilitationsprogramm absolvieren, um seinen Allgemeinzustand und seine körperliche Belastbarkeit zu optimieren.
Methodik: Die Resektion von peripheren Lungensegmenten wird mit Klammernahtapparaten durchgeführt. Eine Verringerung von zirka 30 % des Lungengewebes wird angestrebt. Durch die Resektion der am meisten destruierten Areale verringert sich das Residual- und Gesamtlungenvolumen, das Zwerchfell erhält wieder seine funktionell bessere Wölbung, so daß eine Verbesserung des transdiaphragmentalen Druckaufbaues möglich wird. Studien zeigten bei selektionierten Patienten eine Verbesserung der Lungenfunktion, der Atemmechanik, der Leistungsfähigkeit und der Lebensqualität nach LVRS. Jedoch sind noch einige Fragen hinsichtlich der optimalen Patientenselektion, der Operationstechnik und des Langzeiterfolges offen.
Ergebnisse: An unserer Abteilung wurde die LVRS zwischen September 1994 und Mai 1999 über mediane Sternotomie (n=49), über Thorakotomie (n=18) oder kombiniert über Thorakotomie auf einer Seite und Videoendoskopisch auf der anderen Seite (n=9) bei insgesamt 91 Patienten (Alter 33 bis 80 Jahre, mittleres Alter 56,4 Jahre) durchgeführt. Die perioperative Mortalität betrug 5,5 % (5 Patienten). Die mittlere FeV1 erhöhte sich signifikant um 28,6 % von 25,5±1,2 % des Sollwertes präoperativ auf 32,8±1,9 % des Sollwertes innerhalb der ersten 6 Monate postoperativ (p<0,05). Das mittlere RV sank von 320,3 ±7,91 % des Sollwertes präoperativ auf 248,4±7,5 % des Sollwertes 6 Monate postoperativ und die mittlere TLC von 140,2 ± 2,4 % des Sollwertes auf 126,1±2,1 (p<0,05). Der intrinsische PEEP sank signifikant von 5,1±0,4 cm H2O präoperativ auf 2,3 ±0,3 cm H2O postoperativ (p < 0,5).
Schlußfolgerungen: Diese Ergebnisse deuten darauf hin, daß LVRS eine ausgezeichnete therapeutische Option bei selektionierten Patienten mit schwerem Emphysem und zusätzlichem Zeichen einer schweren Überblähung ist. LVRS bietet die Möglichkeit einer signifikanten postoperativen funktionellen Verbesserung und einer deutlichen Steigerung der Lebensqualität.
Similar content being viewed by others


References
Argenziano M, Moazimi N, Thomashaw B, et al: Extended indications for volume reduction pneumectomy in advanced emphysema. Presented at the 32nd Annual Meeting of The Society of Thoracic Surgeons. Orlando, FL, Jan 29–31, 1996.
Brantigan OC, Mueller E, Kress MB: A surgical approach to pulmonary emphysema. Am Rev Respir Dis 1959; 80: 194–202.
Connoly JE, Wilson A: The current status of surgery for bullous emphysema. J Thorac Cardiovasc Surg 1989; 97: 351–361.
Cooper JE: The history of surgical procedures for emphysema. Ann Thorac Surg 1997; 63: 312–319.
Cooper JD, Patterson GA, Sundaresan RS, et al: Results of 150 consecutive bilateral lung volume reduction procedures in patients with severe emphysema. J Thorac Cardiovasc Surg 1996; 112: 1319–1330.
Cooper JD, Patterson GA: Lung-volume reduction surgery for severe emphysema. Chest Surg Clin N Am 1995; 5: 815–831.
Cooper JD, Trulock EP, Triantafillou AN, Patterson GA, Deloney PA, Sundaresan RS, Roper CL: Bilateral pneumectomy (volume reduction) for chronic obstructive pulmonary disease. J Thorac Cardiovasc Surg 1995; 109: 106–119.
Eugene J, Ott RA, Gogia HS, et al: Video-thoracic surgery for treatment of end-stage bullous emphysema and chronic obstructive pulmonary disease. Am Surg 1995;61:934–936.
Gaensler EA, Gaensler EHL: Surgical treatment of bullous emphysema. In Glenn’s Thoracic and Cardiovascular Surgery. 5th ed. Appleton and Lange, 1991, pp 193–217.
Gaissert H, Trulock EP, Sundaresan S, et al: Comparison of early functional results after volume reduction or transplantation for COPD. J Thorac Cardiovasc Surg 1996; 111: 296–307.
Keenan RJ, Lanreneau RJ, Sciurba FC, et al: Unilateral thoracoscopic surgical appraoch for diffuse emphysema. J Thorac Cardiovasc Surg 1996; 111: 308–316.
McKenna RJ jr, Brenner M, Gelb AF, et al: A randomized, prospective trial of stapled lung reduction versus laser bullectomy for diffuse emphysema. J Thorac Cardiovasc Surg 1996; 111: 317–322.
McKenna RJ, Brenner M, Fischel RY, Gelb AF: Should lung reduction surgery for emphysema be unilateral or bilateral? J Thorac Cardiovasc Surg (in press).
Miller JI jr, Lee RB, Mansour KA: Lung volume reduction surgery: lessons learned for emphysema. Ann Thorac Surg 1996; 61: 1464–1469.
Naunheim KS, Ferguson MK: The current status of Lung Volume Reduction operations for emphysema. Ann Thorac Surg 1996; 62: 601–612.
Naunheim KS, Keller CA, Krucylak PE, et al: Unilateral VATS lung reduction. Ann Thorac Surg 1996; 61: 1092–1098.
Tschernko EM, Wisser W, Hofer S, et al: Influence of lung volume reduction on ventilatory mechanics in patients suffering from severe COPD. Anesth Analg 1996; 83: 996–1001.
Wakayabashi A: Thoracoscopic laser pneumoplasty in the treatment of diffuse bullous emphysema. Ann Thorac Surg 1995; 60: 936–942.
Wisser W, Klepetko W, Kontrus M, et al: Morphologic grading of the emphysematous lung and ist relation to improvement after lung volume reduction surgery. Ann Thorac Surg 1998; 65: 793–799.
Wisser W, Tschernko E, Senbaklavaci Ö, et al: Functional improvement after volume reduction: sternotomy versus videoendoscopic approach. Ann Thorac Surg 1997; 63: 822–828.
Zenati M, Keenan RJ, Landreneau RJ, et al: Lung reduction as bridge to lung transplantation in pulmonary emphysema. Ann Thorac Surg 1995; 59: 1581–1583.
Zenati M, Landreneau RJ, Sciurba F, et al: Role of lung reduction in lung transplant candidates with pulmonary emphysema. Presented at the 32nd Annual Meeting of The Society of Thoracic Surgeons, Orlando, FL, Jan 29–31, 1996.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Senbaklavaci, Ö., Wisser, W., Özpeker, C. et al. Lung volume reduction surgery in patients with emphysema. Acta Chir Austriaca 31, 302–307 (1999). https://doi.org/10.1007/BF02619930
Issue Date:
DOI: https://doi.org/10.1007/BF02619930
Key words
- Lung volume reduction surgery
- diffuse emphysema
- global respiratory failure
- alpha-1-antitrypsin deficiency