
Abstract
In a retrospective study, the clinical course of 250 patients subjected to 257 transverse colostomies was reviewed in an effort to evaluate the problems associated with proximal fecal diversion. Morbidity following stomal construction was 28 per cent, with a significant increase when performed in infants or as an emergency. Two-thirds of the colostomies were emergencies, chiefly due to obstruction and free perforation which was associated with a mortality rate of 12 and 48 per cent respectively.
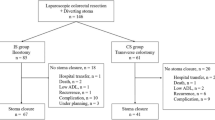
In 102 patients undergoing definite colorectal resection with a previous or simultaneous transverse colostomy, the overall morbidity rate was 58 per cent including a leakage rate of 22.5 per cent. Despite a proximal defunctioning colostomy, surgical intervention was required in 12.7 per cent with a fatal outcome due to peritonitis in 3.9 per cent. Colostomy closure was associated with a morbidity rate of 57 per cent, comprising a leakage rate of 10 per cent and a mortality rate of 1.7 per cent.
Apart from incurable cancer and deaths prior to closure every third patient kept the transverse colostomy permanently. Advanced age and poor condition of patients not proceeding to a definite treatment, or an underlying benign lesion were the three most determining factors. The present results indicate a too extensive use of transverse colostomy, emphasizing the need for a circumspect initial selection of patients for diversionary procedures.
Similar content being viewed by others


References
Colcock BP. Recent experience in the surgical treatment of diverticulitis. Surg Gynecol Obstet 1965;121:63–9.
Goligher JC, Graham NG, De Dombal FT. Anastomotic dehiscence after anterior resection of rectum and sigmoid. Br J Surg 1970;57:109–18.
Smithwick RH. Surgical treatment of diverticulitis of the sigmoid. Am J Surg 1960;99:192–205.
Debas HT, Thomson FB. A critical review of colectomy with anastomosis. Surg Gynecol Obstet 1972;135:747–52.
Fielding LP, Stewar-Brown S, Blesovsky L. Large-bowel obstruction caused by cancer: a prospective study. Br Med J 1979;2:515–7.
Høier-Madsen K, Bech Hansen J, Lindenberg J. Anastomotic leakage following resection for cancer of the colon and rectum. Acta Chir Scand 1975;141:304–9.
Schrock TR, Deveney CW, Dunphy JE. Factors contributing to leakage of colonic anastomoses. Ann Surg 1973;513–8.
Beck PH, Conklin HB. Closure of colostomy. Ann Surg 1975;181:795–8.
Dolan PA, Caldwell FT, Thompson CH, Westbrook KC. Problems of colostomy closure. Am J Surg 1979;137:188–91.
Finch DR. The results of colostomy closure. Br J Surg 1976;63:397–9.
Knox AJ, Birkett FD, Collins CD. Closure of colostomy. Br J Surg 1971;58:669–72.
Mirelman D, Corman ML, Veidenheimer MC, Coller JA. Colostomie—indications and contraindications: Lahey Clinic experience, 1963–74. Dis Colon Rectum 1978; 21:172–6.
Mitchell WH, Kovalcik PJ, Cross GH. Complications of colostomy closure. Dis Colon Rectum 1978;21:180–2.
Smit R, Walt AJ. The morbidity and cost of the temporary colostomy. Dis Colon Rectum 1978;21:558–61.
Thomson JP, Hawley PR. Results of closure of loop transverse colostomies. Br Med J 1972;3:459–62.
Todd GJ, Kutcher LM, Markowitz AM. Factors influencing the complications of colostomy closure. Am J Surg 1979; 137:749–51.
Wheeler MH, Barker J. Closure of colostomy—a safe procedure? Dis Colon Rectum 1977;20:29–32.
Yajko RD, Norton LW, Bloemendal L, Eiseman B. Morbidity of colostomy closure. Am J Surg 1976;132:304–6.
Yakimets WW. Complications of closure of loop colostomy. Can J Surg 1975;18:366–70.
Burns FJ. Complications of colostomy. Dis Colon Rectum 1970;13:448–9.
Green EW. Colostomies and their complications. Surg Gynecol Obstet 1966;122:1230–2.
Hines JR, Harris GD. Colostomy and colostomy closure. Surg Clin North Am 1977;57:1279–92.
Saha SP, Rao N, Stephenson SE Jr. Complications of colostomy. Dis Colon Rectum 1973;16:515–6.
Bacon HF, Herabat T, Tse Gn, Koohdary A. Is colostomy a necessary complement to elective left colonic resection? Dis Colon Rectum 1973;16:29–32.
Balz J, Samson RB, Stewart WR. Rectal-tube decompression in left colectomy. Dis Colon Rectum 1978; 21:94–7.
Garnjobst W, Leaverton GH, Sullivan ES. Safety of colostomy closure. Am J Surg 1978;136:85–9.
Goldstein M, Duff JH. Reconsideration of colostomy in elective left colon resection. Surg Gynecol Obstet 1972;134:593–4.
Hubbard TB Jr, Norico A, Harris RA. Two stage resection of the colon. Surg Gynecol Obstet 1967;124:1081–3.
Botsford TW, Zollinger RM Jr, Hicks R. Mortality of the surgical treatment of diverticulitis. Am J Surg 1971;121:702–5.
Gallagher DM, Russell TR. Surgical management of diverticular disease. Surg Clin North Am 1978;58:563–72.
Graves HA Jr, Franklin RM, Robbins LB II, Sawyers JL. Surgical management of perforated diverticulitis of the colon. Am Surg 1973;39:142–7.
Howe JH, Casali RE, Westbrook KC, Thompson BW, Read RC. Acute perforations of the sigmoid colon secondary to diverticulitis. Am J Surg 1979;137:184–7.
Rodkey GV, Welch CE. Colonic diverticular disease with surgical treatment: a study of 338 cases. Surg Clin North Am 1974;54:655–74.
Carboni R. The treatment of acute left colon obstruction due to cancer. Chir Gastroenterol 1978;12:53–9.
Hughes ES. Mortality of acute large-bowel obstruction. Br J Surg 1966;53:593–4.
Irvin TT, Greaney MG. The treatment of colonic cancer presenting with intestinal obstruction. Br J Surg 1977;64:741–4.
Praderi R, Delgado B, Maquieira G, Aguiar A, Mazza M. Emergency resection for acute neoplastic obstruction of left colon. Chir Gastroenterol 1974;8:291–8.
Valerio D, Jones PF. Immediate resection in the treatment of large bowel emergencies. Br J Surg 1978;65:712–6.
Wright HK. Improving transverse colostomy function. Am J Surg 1979;137:475–7.
Author information
Authors and Affiliations
About this article
Cite this article
Wara, P., Sørensen, K. & Berg, V. Proximal fecal diversion: Review of ten years' experience. Dis Colon Rectum 24, 114–119 (1981). https://doi.org/10.1007/BF02604299
Received:
Issue Date:
DOI: https://doi.org/10.1007/BF02604299