
Abstract
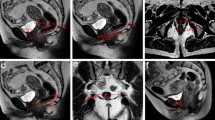
The aim of this study was to determine whether low-field magnetic resonance (MR) imaging can safely and accurately depict inflammatory changes in patients with anal dynamic graciloplasty, in whom high-field MR imaging is contraindicated and ultrasonography and computed tomography are inadequate. A 0.2-T field-strength MR examination was performed in six patients with anal dynamic graciloplasty malfunction in whom reoperation was contemplated. The following sequences were applied:T 2-weighted turbo spinecho with fat saturation,T 1-weighted conventional spin-echo, and contrastenhancedT 1-weighted conventional spin-echo with fat saturation. Results indicated that none of the patients experienced relevant discomfort, pacemaker malfunction, or electrode dislocation with low-field MR imaging. Inflammatory pelvic changes were visualized in four patients and atrophy of the transposed gracilis muscle in another. Surgery was thus avoided in the four, who underwent conservative treatment for their pelvic inflammation. It was concluded that these prelininary results demonstrate the feasibility of MR imaging with a low field strength in patients with anal dynamic graciloplasty. In such patients, in whom diagnostic imaging had been problematic, the potential for safe and accurate visualization will be a boon to treatment planning.
Similar content being viewed by others


References
Cavina E, Seccia M, Evangelista G. Perineal colostomy and electrostimulated gracilis ‘neosphincter’ after abdomino-perineal excision of the colon and anorectum: a surgical experience and follow-up study in 47 cases. Int J Colorectal Dis 1990;5:6–11.
Baeten CG, Konsten J, Spaans F, et al. Dynamic graciloplasty for treatment of faecal incontinence. Lancet 1991;338:1163–5.
Williams NS, Patel J, George BD, Hallan RI, Watkins ES. Development of an electrically stimulated neoanal sphincter. Lancet 1991;338:1166–9.
Baeten CG, Geerdes BP, Adang EMM, et al. Anal dynamic graciloplasty in the treatment of intractable fecal incontinence. N Engl J Med 1995;332:1600–5.
Sommer T, Lauck G, Schimpf R, et al. Magnetic resonance imaging in patients with cardiac pacemakers: in vitro- and in vivo-evaluation at 0.5 T. Fortschr Roentgenstr 1998;168:36–43.
Alagona P, Toole J, Maniscalco B, Glover MU, Abernathy GT, Prida XE. Nuclear magnetic resonance imaging in a patient with a DDD pacemaker. Pacing Clin Electrophysiol 1989;12:619.
Inbar S, Larson J, Burt T, Mafee M, Ezri MD. Nuclear magnetic resonance imaging in a patient with a pacemaker. Am J Med Sci 1993;305:174–5.
Liem LA, Van Dongen VCPC. Magnetic resonance imaging and spinal cord stimulation systems. Pain 1997;70:95–7.
Pickrell KL, Broadbent TR, Masters FW, Metzger JT. Construction of a rectal sphincter and restoration of anal continence by transplanting the gracilis muscle: a report of four cases in children. Ann Surg 1952;135:853–62.
Yoshioka K, Keighley MR. Clinical and manometric assessment of gracilis muscle implant for faecal incontinence. Dis Colon Rectum 1988;31:767–9.
Konsten J, Baeten CG, Spaans F, Havenith MG, Soeters PB. Follow-up of anal dynamic graciloplasty for fecal continence. World J Surg 1993;17:404–9.
George BD, Williams NS, Patel J, Swash M, Watkins ES. Physiological and histochemical adaptation of the electrically stimulated gracilis muscle to neoanal sphincter function. Br J Surg 1993;80:1342–6.
Geerdes BP, Zoetmulder FAN, Baeten CGMI. Double dynamic graciloplasty and coloperineal pull-through after abdominoperineal resection. Eur J Cancer 1995;31:1248–52.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Cavallaro, A., Fellner, F., Matzel, K.E. et al. Low-field magnetic resonance imaging of the pelvis in patients with anal dynamic graciloplasty: initial experience. MAGMA 7, 179–183 (1998). https://doi.org/10.1007/BF02591335
Received:
Revised:
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF02591335