
Abstract
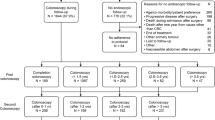
This study investigates the possible gain and limitation by performing colonoscopy and double-contrast enema immediately after, and every six months after, radical surgery for colorectal cancer. It was possible to perform a complete colonoscopy within three months of surgery in 80 per cent of the 239 patients and at the follow-up time in 90 per cent. Incompleteness was related to insufficient bowel preparation, narrow anastomosis, and long transverse colon. Five patients had synchronous cancers, and 64 had adenomas at the time of surgery. The risk of recurrent adenomas in the latter was higher (17/64) than in those without adenomas (15/175). The adenomas were located above the rectum in 57 of 80 patients who had polypectomy. Four patients with metachronous cancer and one of five patients with local recurrence had another radical operation, while this was possible in none of 40 patients with recurrence diagnosed by other means than colonoscopy and enema. Radical colorectal surgery should be followed by colonoscopy and double-contrast enema, but how often and for how long remains to be established.
Similar content being viewed by others


References
Schottenfeld D, Berg JW, Vitsky B. Incidence of multiple primary cancers. J Natl Cancer Inst 1969;43:77–86.
Kronborg O. Polyps of the colon and rectum: approach to prophylaxis in colorectal cancer. Scand J Gastroenterol 1980;15:1–5.
Gilbertsen VA. Proctosigmoidoscopy and polypectomy in reducing the incidence of rectal cancer. Cancer 1974;34:936–9.
Kronborg O, Hage E, Deichgraeber E. The clean colon: a prospective partly randomized study of the effectiveness of repeated examinations of the colon after polypectomy and radical surgery for cancer. Scand J Gastroenterol 1981;16:879–84.
Vassilopoulus PP, Yoon JM, Ledesma EJ, Mittelman A. Treatment of recurrence of adenocarcinoma of the colon and rectum at the anastomotic site. Surg Genecol Obstet 1981;152:777–80.
Balslev I, Pedersen M, Teglbjaerg PSet al. Postoperative radiotherapy in rectosigmoid cancer Dukes B and C—interim report from a randomized multicentre study. Br J Cancer 1982;46:551–556.
Welin S, Welin G. The double contrast examination of the colon: experiences with the Welin modification. Stuttgart: Georg Thieme, 1976.
Frank B, Zeabart LE, Brady PG. Colonoscopic evaluation following partial colon resection for adenocarcinoma (abstr.) Am J Gastroenterol 1979;72:335.
Appel MF. Distribution of malignant polyps in the colon. Gastrointest Endosc 1981;27:119.
Rittenhouse MC, Copeland EM. Carcinoma in situ of the distal part of the colon and of the rectum. Surg Gynecol Obstet 1978; 146:225–9.
Henry LG, Condon RE, Schulte WJ, Aprahamian C, DeCosse JJ. Risk of recurrence of colon polyps. Ann Surg 1975;182:511–5.
Ekman C, Gustavson J, Henning A. Value of a follow-up study of recurrent carcinoma of the colon and rectum. Surg Gynecol Obstet 1977;145:895–7.
Cochrane JPS, Williams JT, Faber RG, Slack WW. Value of out-patient follow-up after curative surgery for carcinoma of the large bowel. Br Med J 1980;1:593–5.
Winawer SJ, Sherlock P. Approach to screening and diagnosis in colorectal cancer. Semin Oncol 1976;3:387–97.
Polk HC, Spratt JS. Recurrent colorectal carcinoma: detection, treatment, and other considerations. Surgery 1971;69:9–23.
Welch JP, Donaldson GA. Detection and treatment of recurrent cancer of the colon and rectum. Am J Surg 1978;135:505–11.
Flick AL. Appearance and growth of colon neoplasms in less than two years: nine cases (abstr.) Gastroenterology 1978;74:1035.
Shindo K. Recurrence of carcinoma of the large intestine. Am J Proctol 1974;25:80–90.
Heald RJ, Lockhart-Mummery HE. The lesion of the second cancer of the large bowel. Br J Surg 1972;59:16–9.
Muto T, Bussey HJR, Morson BC. The evolution of cancer of the colon and rectum. Cancer 1975;36:2251–70.
Shinya H, Wolff WI. Morphology, anatomic distribution and cancer potential of colonic polyps. Ann Surg 1979;190:679–83.
Koppel M, Bailar JC III, Weakley FL, Shimkin MB. Incidence of cancer in the colon and rectum among polyp-free patients. Dis Colon Rectum 1962;5:349–55.
Author information
Authors and Affiliations
About this article
Cite this article
Kronborg, O., Hage, E. & Deichgraeber, E. The remaining colon after radical surgery for colorectal cancer. Dis Colon Rectum 26, 172–176 (1983). https://doi.org/10.1007/BF02560165
Received:
Issue Date:
DOI: https://doi.org/10.1007/BF02560165