
Summary
Goal of surgery
Restoration of joint anatomy to ensure normal development and function of the hip.
Indications
After failed closed reduction of hip dislocation in instances of congenital hip dysplasia or neurologic disorders in children such as cerebral palsy, myelomeningocele.
Contraindications
Untreated superior hip dislocation in adolescents or adults with deformities of the femoral head and acetabulum resulting in joint incongruity.
Preoperative work up
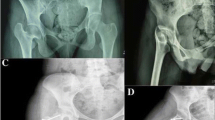
Radiographs of both hips (Rippstein I and II), arthrography. In the presence of deformities or joint incongruities CT-scan with 3-D-reconstruction.
Positioning and anaesthesia
Supine, affected side of pelvis elevated with a roll of towels. General anaesthesia.
Surgical technique
Open reduction of the dislocated femoral head through an anterolateral approach and T-shaped opening of the capsule and removal of any intraarticular obstacles preventing anatomic reduction. Optional tenotomy of iliopsoas muscle and/or adductor muscles. Capsulorraphy.
Postoperative management
In children less than 2 years old: 6 weeks of immobilization in a spica cast.
In children who did not walk preoperatively: Pavlik harness and physiotherapy.
In children who have been able to walk preoperatively: night abduction splint and physiotherapy for 6 months.
In older children or when open reduction was combined with acetabular and femoral osteotomy: spica cast for 1 week, gentle passive exercises during the 2nd week, and abduction splint for another 4 weeks.
Possible complications
Persistence of superior dislocation.
Too extensive incision of the capsule.
Redislocation.
Contracture.
Results
63 patients were operated between 1974 and 1993. Average age at surgery: 1 year, 10 months. Using the classification of Tönnis: 21 patients had a grade II, 23 a grade III and 43 a grade IV dislocation. In 5% of patients a neurologic disorder was present.
Based on the surgical technique used the patients were subdivided into 3 groups: in 26 patients: open reduction only (average age: 20.5 months); in 22 patients: open reduction followed by acetabular and femoral osteotomies at a later date (average age 20 months); in 15 patients: open reduction combined with corrective acetabular and femoral osteotomies (average age: 34 months).
Average follow-up time: 5 years, 10 months, excluding 6 patients, who were operated on within the last year.
Out of 57 patients 45 presented a well centred hip, full range of motion and a normal development of the ossific nucleus (Tönnis grade I).
In 14% of patients avascular necrosis of different degrees was observed.
Similar content being viewed by others


Literatur
Fettweis, E.: Sitz-Hock-Stellungsgips bei Hüftgelenksdysplasien. Arch. orthop. Trauma Surg. 63 (1968), 38–51.
Severin, E.: Contribution to the knowledge of congenital dislocation of the hip joint. Late results of closed reduction and arthrographic studies of recent cases. Acta chir. scand. 84, Suppl. 63 (1941), 1–142.
Severin, E.: Spätresultate unblutiger Behandlung von Luxatio coxae congenita. Z. Orthop. 74 (1943), 52–75.
Tönnis, D.: Die angeborene Hüftdysplasie und Hüftluxation im Kindes- und Erwachsenenalter. Springer, Berlin-Heidelberg-New York-Tokyo 1984.
Tönnis, D.: Hüftluxation und Hüftkopfnekrose. Eine Sammelstatistik des Arbeitskreises für Hüftdysplasie. Bücherei des Orthopäden, Bd. 21. Enke, Stuttgart 1978.
Tönnis, D.: Congenital hip dislocation—avascular necrosis. Necrosis of the femoral head as a complication of different conservative and operative methods of reduction in congenital dislocation of the hip, Thieme —Stratton-New York 1982.
Watson-Jones, R.: Fractures of the neck of the femur. Brit. J. Surg. 23 (1936), 787.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Carstens, C., Schuknecht, B. Die offene Reposition des luxierten Hüftgelenks im Kindesalter. Operat Orthop Traumatol 8, 262–270 (1996). https://doi.org/10.1007/BF02510187
Issue Date:
DOI: https://doi.org/10.1007/BF02510187